When Sjögren’s Mimics Infection: Meningoencephalitis with Acute Motor Axonal Neuropathy
Published in Neuroscience and Biomedical Research
Case Overview
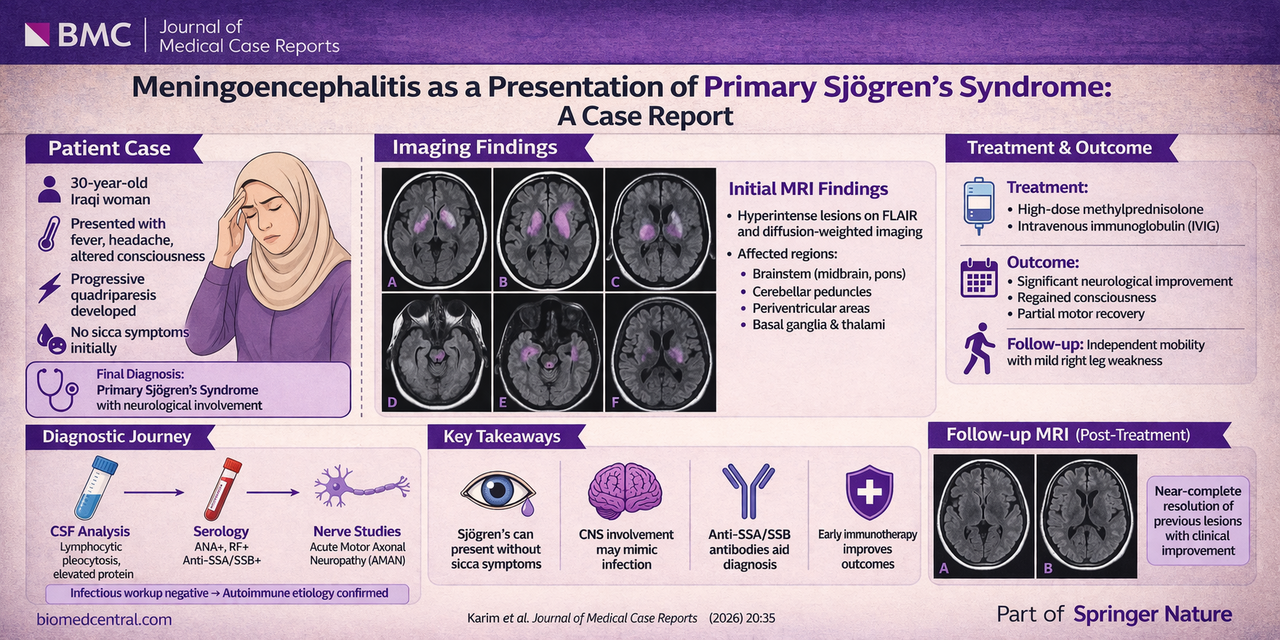
Karim et al. present a compelling case of a 30-year-old woman who developed acute meningoencephalitis with rapid neurological decline, followed by acute motor axonal neuropathy (AMAN), a Guillain–Barré syndrome variant.
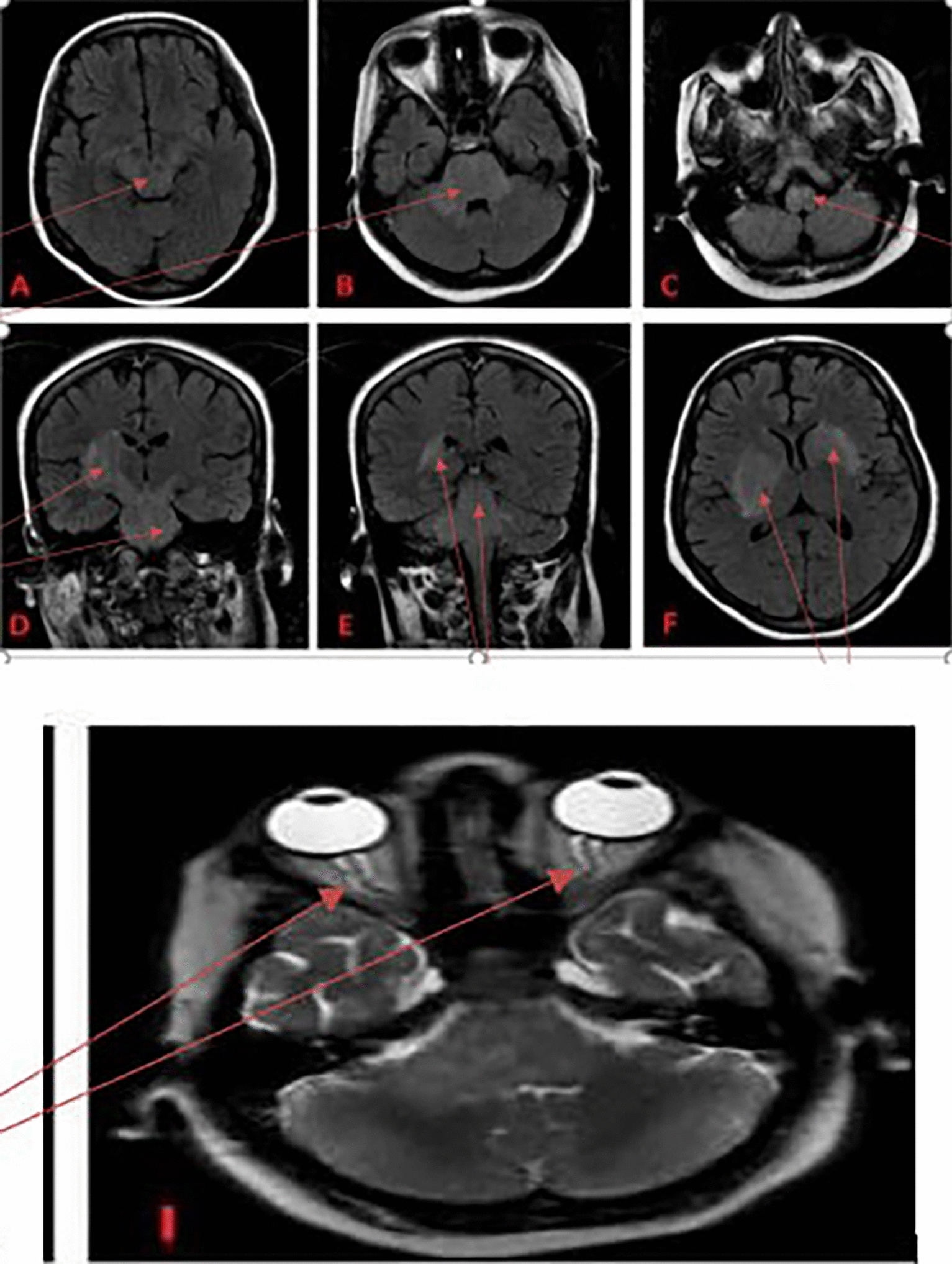
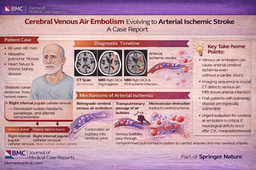
Initial presentation included fever, headache, altered consciousness, and progressive quadriparesis. Cerebrospinal fluid analysis showed lymphocytic predominance and elevated protein, while MRI demonstrated extensive brainstem and deep gray matter hyperintensities on FLAIR and diffusion-weighted imaging, as illustrated in the imaging panels on page 3, involving the midbrain, pons, cerebellar peduncles, basal ganglia, and thalami.
Despite initial treatment for presumed infectious meningoencephalitis, the lack of clinical improvement and negative infectious workup prompted evaluation for autoimmune etiologies. Serologic testing revealed positive ANA, rheumatoid factor, and anti-SSA/SSB antibodies, confirming primary Sjögren’s syndrome. Concurrent nerve conduction studies demonstrated a pure motor axonal neuropathy consistent with AMAN.
The patient was treated with high-dose corticosteroids and intravenous immunoglobulin (IVIG), resulting in substantial neurological recovery. Follow-up imaging (page 5) demonstrated near-complete resolution of prior lesions, paralleling clinical improvement.
Why This Case Matters
This case highlights several important clinical lessons:
Atypical presentation: Sjögren’s syndrome may initially present with CNS inflammation rather than sicca symptoms
Dual pathology: Simultaneous central (meningoencephalitis) and peripheral (AMAN) involvement is rare but possible
Diagnostic pitfall: Early features may closely mimic infectious meningoencephalitis or neuromyelitis optica
Imaging clues: Brainstem and deep gray matter involvement with inflammatory characteristics should raise suspicion for autoimmune etiologies
Therapeutic implications: Prompt immunotherapy can lead to meaningful neurological recovery
Notably, neurological manifestations may precede classic sicca symptoms in up to a substantial proportion of cases, further complicating early diagnosis.
Clinical Take-Home Message
In patients with unexplained meningoencephalitis and concurrent motor neuropathy, particularly when infectious studies are negative, primary Sjögren’s syndrome should be strongly considered, as early immunotherapy can significantly improve outcomes.
Question
Which feature most strongly supports Sjögren’s syndrome as the underlying cause of this patient’s neurological presentation?
A. Brainstem hyperintensities on MRI
B. Lymphocytic cerebrospinal fluid profile
C. Positive anti-SSA and anti-SSB antibodies
D. Acute motor axonal neuropathy
Correct Answer:
C. Positive anti-SSA and anti-SSB antibodies
While MRI findings and CSF abnormalities suggest an inflammatory process, they are nonspecific and can be seen in infectious or other autoimmune conditions. The presence of anti-SSA (Ro) and anti-SSB (La) antibodies provides disease-specific serologic evidence supporting the diagnosis of primary Sjögren’s syndrome, particularly when integrated with the clinical presentation.
Final Thoughts
This case reinforces the protean nature of Sjögren’s syndrome and the importance of maintaining a broad autoimmune differential in atypical neurological presentations. Early recognition is critical—what initially appears to be infection may instead represent a treatable inflammatory disorder with favorable outcomes when appropriately managed.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in