When steroids raise lactate: an unexpected metabolic signal in a stable stroke patient
Published in Neuroscience and Biomedical Research
Explore the Research
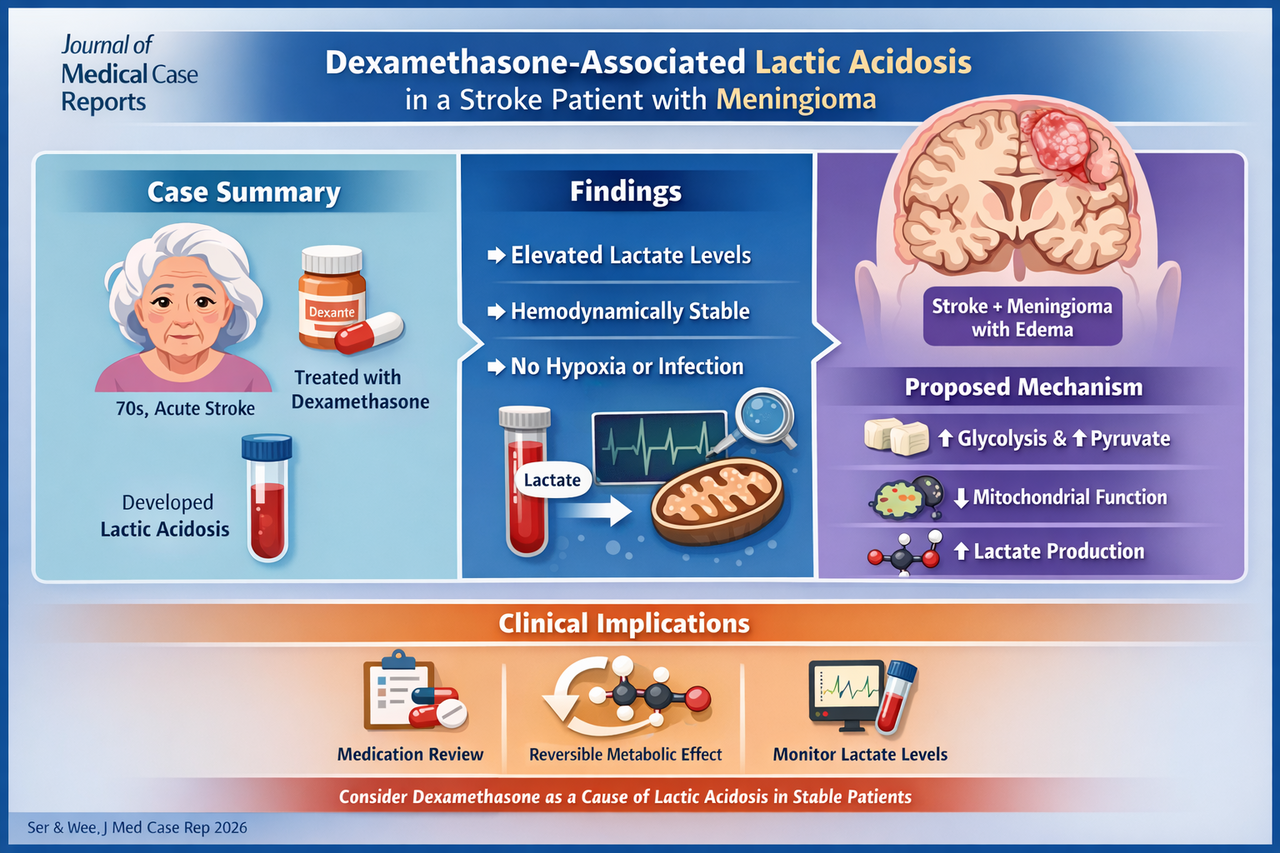
Dexamethasone associated with lactic acidosis in a stroke patient with meningioma-associated vasogenic edema: a case report
Case overview
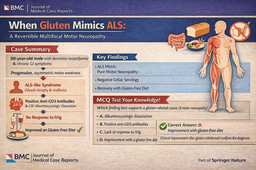
A woman in her 70s presented with an acute right middle cerebral artery stroke and was incidentally found to have a large meningioma with surrounding vasogenic edema. She was started on a tapering course of dexamethasone.
Within days, routine laboratory testing revealed a high anion gap metabolic acidosis, with elevated lactate levels despite:
Hemodynamic stability
No evidence of hypoxia or hypoperfusion
Negative infectious, toxic, and metabolic workup
A systematic evaluation excluded common causes of type A and type B lactic acidosis, ultimately implicating dexamethasone as the likely culprit. Importantly, the patient remained asymptomatic throughout.
Lactate levels peaked at 3.40 mmol/L and normalized within 72 hours of steroid cessation, strongly supporting a drug-induced mechanism .
Mechanistic insight
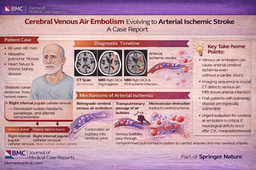
Although the precise mechanism remains uncertain, several biologically plausible pathways emerge:
Enhanced glycolysis and gluconeogenesis → increased pyruvate production
Overflow of pyruvate into anaerobic metabolism → lactate accumulation
Possible mitochondrial dysfunction and ROS-mediated effects impairing oxidative metabolism
Interestingly, this case suggests a duration-dependent rather than dose-dependent relationship, raising important considerations for prolonged steroid use.
Why this case matters
Even mild lactate elevation carries prognostic significance, with increased short- and long-term mortality across hospitalized populations. Yet, corticosteroids are not routinely considered in the differential diagnosis of lactic acidosis—particularly in stable, non-ICU patients.
This report expands the clinical context in which steroid-associated hyperlactatemia may occur and underscores the importance of:
Careful medication reconciliation
Avoiding unnecessary escalation of sepsis workups
Recognizing reversible, drug-induced metabolic derangements
Clinical pearl
In patients with unexplained lactic acidosis—especially when clinically stable—review corticosteroid exposure as a potential cause of type B lactic acidosis.
Question
Which of the following best explains dexamethasone-associated lactic acidosis?
A. Direct inhibition of lactate dehydrogenase
B. Increased glycolysis with excess pyruvate shunting to lactate
C. Renal tubular acidosis
D. Impaired hepatic lactate clearance due to cirrhosis
Correct answer: B
Explanation: Corticosteroids enhance glucose metabolism, increasing pyruvate production. When mitochondrial oxidative capacity is exceeded or impaired, excess pyruvate is converted to lactate, leading to type B lactic acidosis.
Take-home message
This case reinforces a classic principle with a modern nuance:
not all lactic acidosis signals hypoperfusion—sometimes, it reflects pharmacologic metabolism.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in