When strengthening the cornea became a way to fight infection
Published in Microbiology and General & Internal Medicine

Our paper, “Anti-infectious cross-linking: when and how? PACK-CXL as a treatment option for infectious keratitis” brings together the evidence behind this development and asks a practical question: when a corneal infection is threatening vision, how can light, a photosensitive molecule and the cornea’s own tissue be used as part of the treatment?
The clinical problem behind the paper
Infectious keratitis is an infection of the cornea, the transparent tissue at the front of the eye. Bacteria, fungi or other microorganisms, including Acanthamoeba, can cause it. Without prompt and effective treatment, the infection can destroy corneal tissue, leave a dense scar, perforate the eye or result in permanent visual loss.
Conventional treatment usually depends on antimicrobial eye drops. These may need to be applied very frequently, sometimes every hour, for days or weeks. Treatment can become difficult when the microorganism is resistant, when laboratory identification takes time, when drugs penetrate the tissue poorly, or when the patient cannot obtain or reliably use the medication.
These challenges are particularly severe in regions where access to laboratories, specialist ophthalmologists and antimicrobial drugs is limited. However, treatment failure also occurs in highly developed healthcare systems, especially with fungal, resistant or unusually aggressive infections.
Our interest in PACK-CXL emerged from a simple observation: corneal cross-linking was already doing more than strengthening tissue.
From keratoconus to infection
Corneal cross-linking was introduced to slow the progression of keratoconus, a condition in which the cornea becomes mechanically weak, progressively thinner and more irregular.
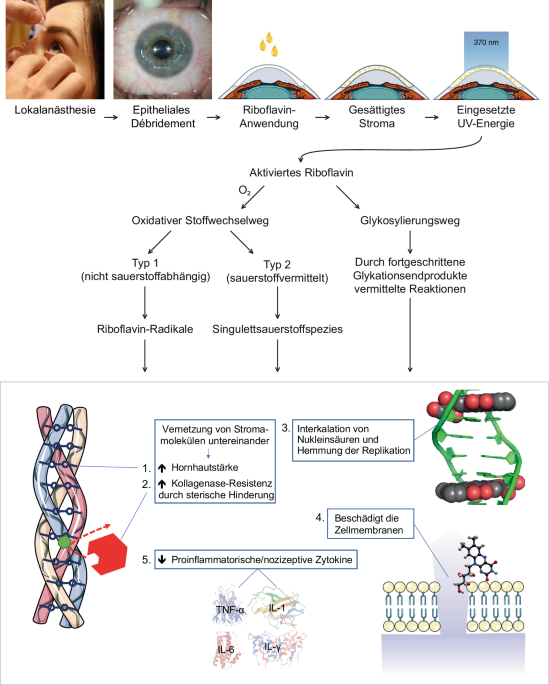
During conventional cross-linking, the cornea is saturated with riboflavin, a form of vitamin B2, and illuminated with ultraviolet-A light. This photochemical reaction generates reactive oxygen species. These short-lived molecules create additional chemical bonds within the corneal tissue, increasing its resistance to deformation.
However, reactive oxygen species also damage microorganisms. They can disrupt microbial cell membranes and interfere with DNA and RNA, preventing replication. At the same time, cross-linking changes the architecture of the corneal collagen matrix, making it more difficult for pathogen-derived enzymes to digest the tissue.
The treatment therefore addresses two components of infectious keratitis at once: the microorganism itself and the corneal destruction caused by its enzymes.
When cross-linking is used for infection rather than ectasia, it is termed photoactivated chromophore for keratitis-corneal cross-linking, or PACK-CXL.
The first clinical clues
The first clinical report appeared in 2008. Five eyes with bacterial or fungal corneal ulcers had continued to deteriorate despite intensive antimicrobial treatment. After conventional riboflavin/UV-A cross-linking, corneal melting was stopped in four of the five eyes.
This was a very small series, but it established an important principle: the photochemical reaction used to stabilize keratoconus might also interrupt a destructive infectious process.
Later studies investigated PACK-CXL as an addition to antimicrobial therapy. A systematic review involving 46 studies and 435 patients found evidence of faster healing and more rapid resolution of corneal infiltrates when PACK-CXL was added to conventional treatment.
The more challenging question was whether PACK-CXL could work without antimicrobial drugs.
An international randomized Phase III study compared standard antimicrobial therapy with PACK-CXL alone in patients with small, relatively superficial bacterial or fungal ulcers. In the PACK-CXL group, 89% of eyes healed without antimicrobial medication, compared with 93% in the conventional-treatment group. Two PACK-CXL-treated eyes required additional antimicrobial treatment. In the medication group, three eyes developed severe structural complications requiring corneal transplantation.
These results do not mean that PACK-CXL should replace antimicrobial therapy in every patient. They do, however, suggest that a single procedure can control selected infections, an observation with major implications where medications, follow-up and patient compliance cannot be assumed.
Why the original protocol was not enough
One of the central themes of our paper is that PACK-CXL should not simply copy the protocol developed for keratoconus.
The infected cornea is often swollen, opaque and infiltrated with inflammatory material. Riboflavin also absorbs ultraviolet light strongly. Consequently, much of the applied energy is absorbed near the corneal surface, leaving progressively less energy available at greater depths.
This matters because microorganisms may be located well below the surface. A UV dose that is sufficient to strengthen a transparent keratoconic cornea may be insufficient to treat a deeper, opaque ulcer.
Laboratory work showed that increasing the total energy dose, or fluence, improves bacterial killing. This helped move PACK-CXL beyond the traditional 5.4 J/cm² “Dresden” protocol towards higher-fluence approaches, commonly beginning at 7.2 J/cm² and, in experimental work, extending further.
The distinction between biomechanical cross-linking and antimicrobial cross-linking is also important. Rapid UV delivery can reduce the biomechanical effect because oxygen is depleted during the reaction. By contrast, bacterial killing appears to be much less dependent on oxygen. PACK-CXL can therefore be accelerated, delivering the required fluence over a few minutes rather than 30 minutes.
For a patient with a painful corneal ulcer, reducing treatment from half an hour to several minutes is not a minor practical improvement.
Different organisms may require different strategies
PACK-CXL is not a single universal protocol.
Small, superficial bacterial ulcers currently have the strongest clinical evidence. Deeper ulcers may require higher fluence because less light reaches the microorganisms. Fungal infections remain more difficult and may require repeated treatment or combination therapy.
Acanthamoeba keratitis is particularly challenging. Neither riboflavin/UV-A nor rose bengal/green-light treatment alone has demonstrated consistently reliable activity against both trophozoites and cysts.
A potential solution is sequential dual-chromophore treatment: riboflavin activated by UV-A, followed during the same session by rose bengal activated with green light. Because the two chromophores absorb different wavelengths, they may produce complementary photochemical effects. An initial clinical case produced an encouraging result after a year of unsuccessful conventional therapy, but this approach still requires prospective clinical validation.
Why we wrote this review now
The PACK-CXL literature has reached an important transitional stage. The biological rationale is well supported, clinical evidence now extends beyond isolated case reports, and practical protocols are becoming shorter and more adaptable.
At the same time, substantial questions remain. The only Phase III trial included 42 eyes and was restricted to ulcers smaller than 4 mm and shallower than 300 μm. Larger, deeper and more advanced infections have not yet been adequately examined in randomized trials. The ideal fluence for different ulcer depths and organisms is also not fully established, and very high fluences require continued safety evaluation.
Our aim was therefore not to present PACK-CXL as a finished treatment algorithm. It was to organize what is currently known into a clinically useful framework while identifying where evidence remains insufficient.
Beyond the operating theatre
One of the most important aspects of this story is accessibility.
Portable UV devices can be attached to a slit lamp, allowing PACK-CXL to be performed outside an operating theatre. This makes it possible to consider treatment in outpatient clinics and regions with limited surgical infrastructure.
In well-resourced settings, PACK-CXL may serve primarily as an adjunct that accelerates healing or helps control resistant infection. In resource-limited settings, a single, largely pathogen-independent procedure could provide treatment when prolonged medication and follow-up are unrealistic.
That does not remove the need for diagnosis, clinical judgement or antimicrobial drugs. It does, however, challenge the assumption that advanced infection treatment must always depend on identifying the organism first and administering organism-specific medication for an extended period.
The broader lesson from PACK-CXL is that technologies often develop beyond their original purpose. Corneal cross-linking began as a method for strengthening weakened tissue. Its photochemistry then revealed another possibility: simultaneously attacking microorganisms and protecting the tissue they are trying to destroy.
The next stage will require larger trials, individualized protocols and careful evaluation of which patients benefit most. But the underlying concept is now difficult to ignore: in selected corneal infections, light may become part of the antimicrobial armamentarium.
Follow the Topic
-
Die Ophthalmologie is an internationally recognized journal dealing with all aspects of ophthalmology. The journal serves both the scientific exchange and the continuing education of ophthalmologists.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in