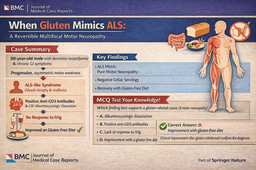
When Venous Air Becomes Arterial Stroke: A Hidden Catastrophe After Central Line Removal
Published in Neuroscience and Biomedical Research
Case Overview
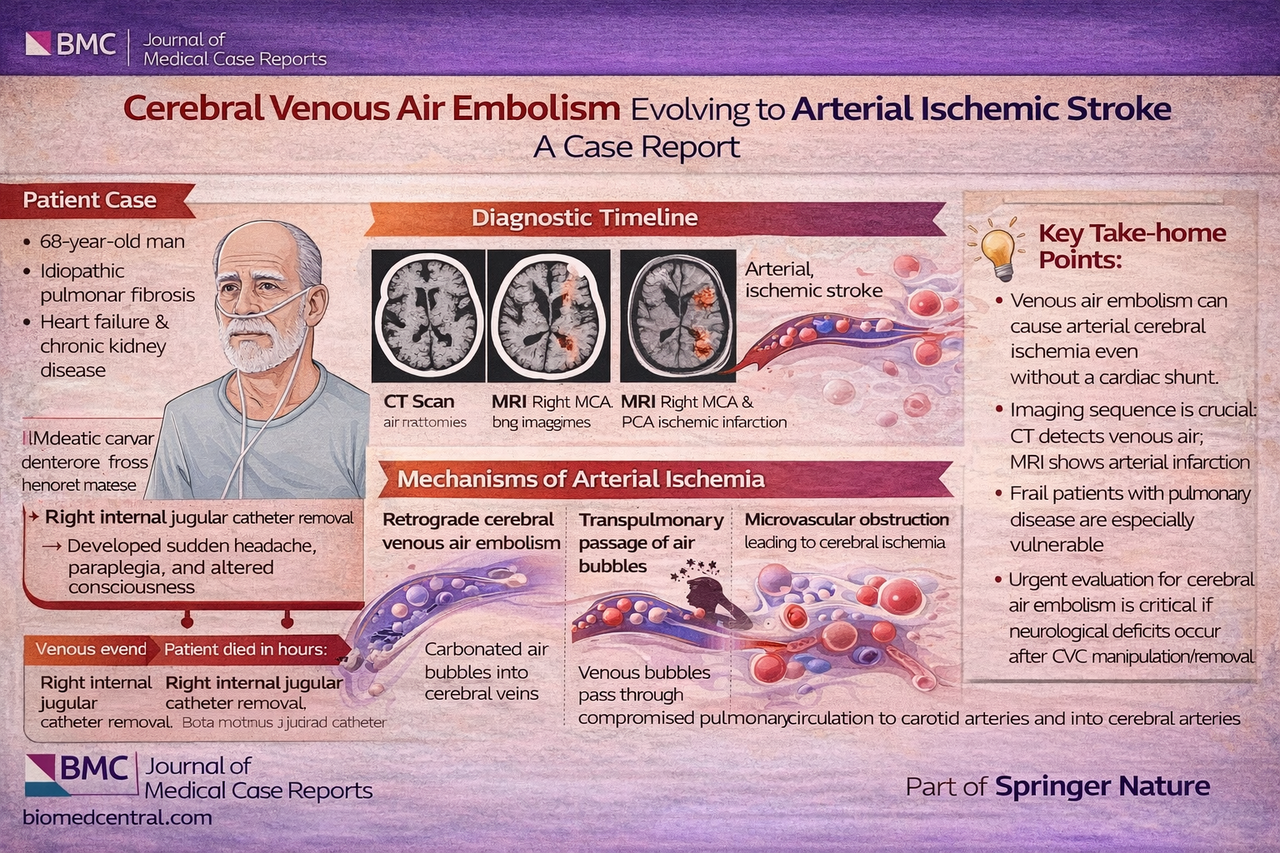
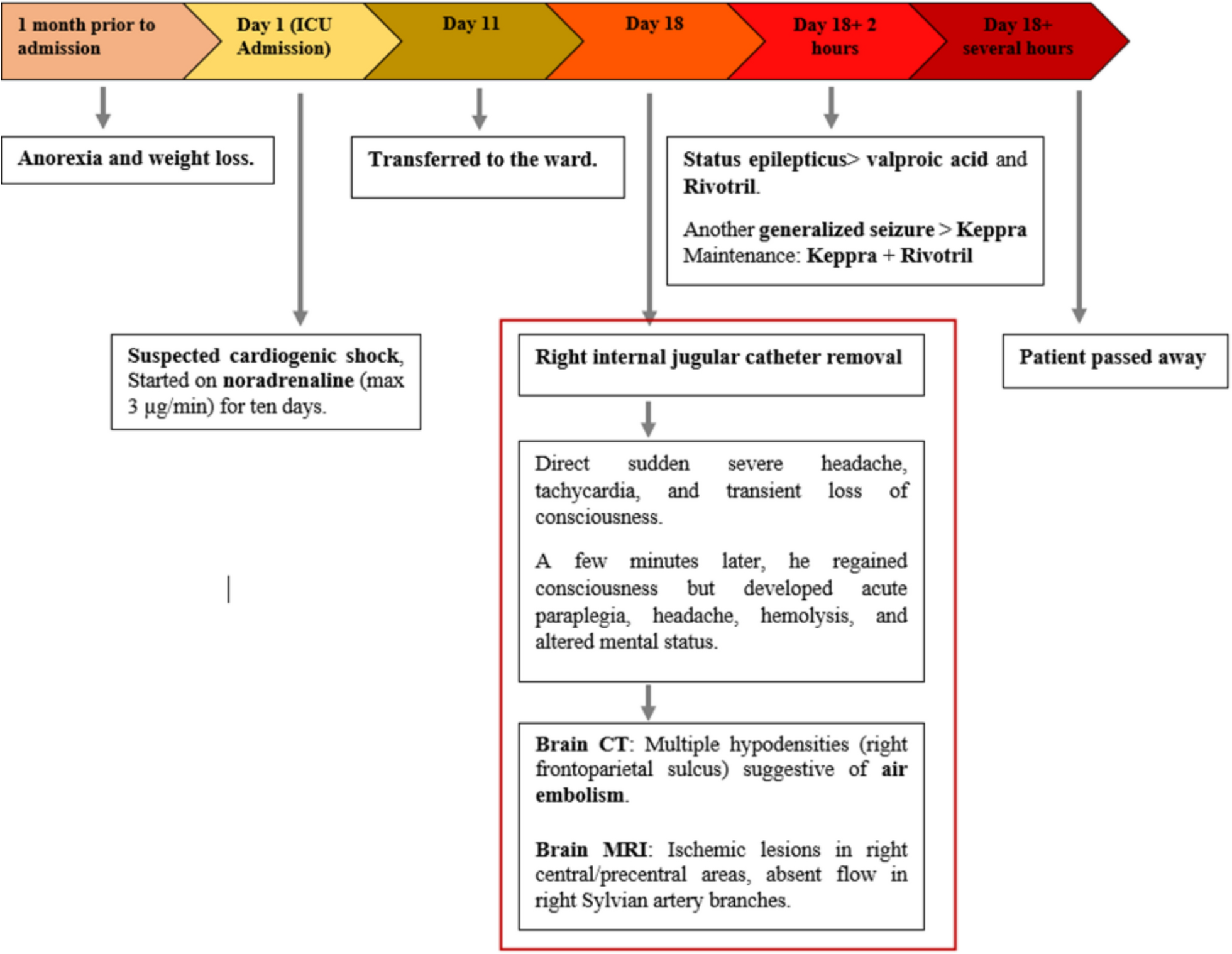
A 68-year-old man with significant comorbidities, including idiopathic pulmonary fibrosis, heart failure, and chronic kidney disease, developed acute neurological collapse immediately following removal of a right internal jugular central venous catheter.
Within minutes, he experienced sudden headache, altered consciousness, and paraplegia, followed by focal neurological deficits. Brain CT demonstrated multiple cortical venous air emboli, visualized as serpiginous hypodensities along the frontoparietal sulci. Subsequent MRI revealed extensive ischemic infarction in the right middle and posterior cerebral artery territories.
Despite prompt supportive management—including high-flow oxygen and antiseizure therapy—the patient deteriorated rapidly, developing refractory status epilepticus and ultimately died following a goals-of-care transition.
Why This Case Matters
This case underscores several critical and practice-changing insights:
Venous air is not always benign—it can serve as a precursor to devastating arterial cerebral ischemia
No intracardiac shunt required—transpulmonary passage or overwhelmed pulmonary filtration may allow arterial embolization
Retrograde cerebral venous air embolism is likely underrecognized, particularly with internal jugular access
High-risk patients (frailty, pulmonary disease, prolonged catheter dwell time) are especially vulnerable
Imaging sequence is key—CT may capture venous air, while MRI later reveals arterial infarction
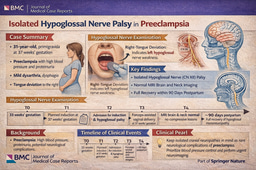
Notably, the timeline on page 3 clearly illustrates the rapid progression from catheter removal to neurological collapse and death within hours, emphasizing the fulminant nature of this complication.
Mechanistic Insight
This case provides compelling support for a venous-to-arterial injury cascade, likely involving:
Retrograde ascent of air into cerebral venous circulation
Transpulmonary passage of microbubbles
Microvascular obstruction and endothelial injury leading to ischemia
Importantly, a negative bubble study does not exclude clinically significant arterial consequences, particularly in patients with impaired pulmonary filtration capacity.
Clinical Take-Home Message
Acute neurological deterioration immediately following CVC manipulation or removal should prompt urgent evaluation for cerebral air embolism, even in the absence of classic risk factors or intracardiac shunt.
Question
Which mechanism best explains arterial cerebral infarction following venous air embolism in the absence of a cardiac shunt?
A. Direct arterial catheterization
B. Retrograde venous flow alone
C. Transpulmonary passage of air bubbles
D. Septic embolization
Correct Answer: C. Transpulmonary passage of air bubbles
Explanation: When pulmonary filtration is impaired—as in pulmonary fibrosis—venous air emboli can traverse the pulmonary circulation and enter the arterial system. Additionally, large embolic loads may overwhelm normal filtration mechanisms, allowing systemic dissemination and cerebral ischemia despite a negative bubble study.
Final Thoughts
This case serves as a sobering reminder that even routine procedures such as central line removal can precipitate catastrophic neurological outcomes. Vigilance, risk stratification, and meticulous technique remain essential—but equally important is early recognition of this rare, often fatal complication.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in