X chromosome associated with Lewy body dementia risk in females
Published in Genetics & Genomics and General & Internal Medicine
Lewy body dementia is an umbrella term for Parkinson’s disease dementia and dementia with Lewy bodies. Both of these diseases have underlying Lewy body pathology and cognitive impairment that affects daily life. Although Lewy body dementia is a common type of dementia following Alzheimer’s and vascular dementia, we do not hear much about it. Research is limited and we still have a lot of unknowns. So far, we have been able to pinpoint some genetic risk factors (including APOE, GBA, SNCA) and a role for sex. Females do not get the pure Lewy body pathology as often as males, and females with Lewy body pathology do not present with the typical clinical profile we associate with Lewy body dementia. Since both the pathology prevalence and association with the clinical features differ by sex, this suggested to us that the risk factors perhaps differ as well.
With sex taking on such a striking role in Lewy body dementia, we wondered how the X chromosome comes into play for risk. The X chromosome is a big part of the genetic story; however, it often gets excluded from genome-wide association studies because of the different quality control measures it requires. With the development of the X chromosome-wide association study pipeline, we wanted to address the gap of knowledge in Lewy body dementia by diving into the world of the X chromosome. Knowing that rare variants also make up a part of the genetic story that often does not get told, we wanted to include them in our analysis as well.
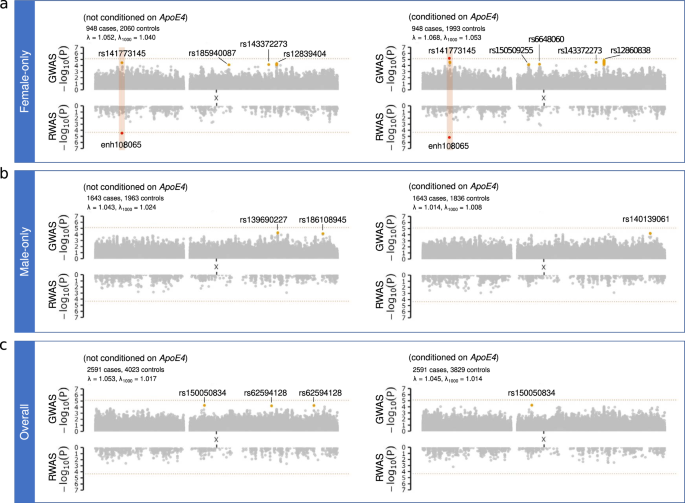
Unfortunately, harmonized data from multiple centers including a large number of people are not too easy to come by in Lewy body dementia. The International Lewy Body Dementia Genetics Consortium has been putting a lot of effort into gathering data and accelerating genetic discoveries in Lewy body dementia. Recently, our group investigated the risk factors for Lewy body dementia with genome genome-wide association study in the compiled data including 2,591 people with Lewy body dementia and 4,391 people without any significant neurological diseases. We leveraged the same cohort in this X chromosome focused study. We performed the X chromosome-specific quality control and then performed analyses in the whole cohort, as well as individually for females and males. We also adjusted the analysis for APOEe4, given the large effect size associated with this factor that can swipe out other potential hits.
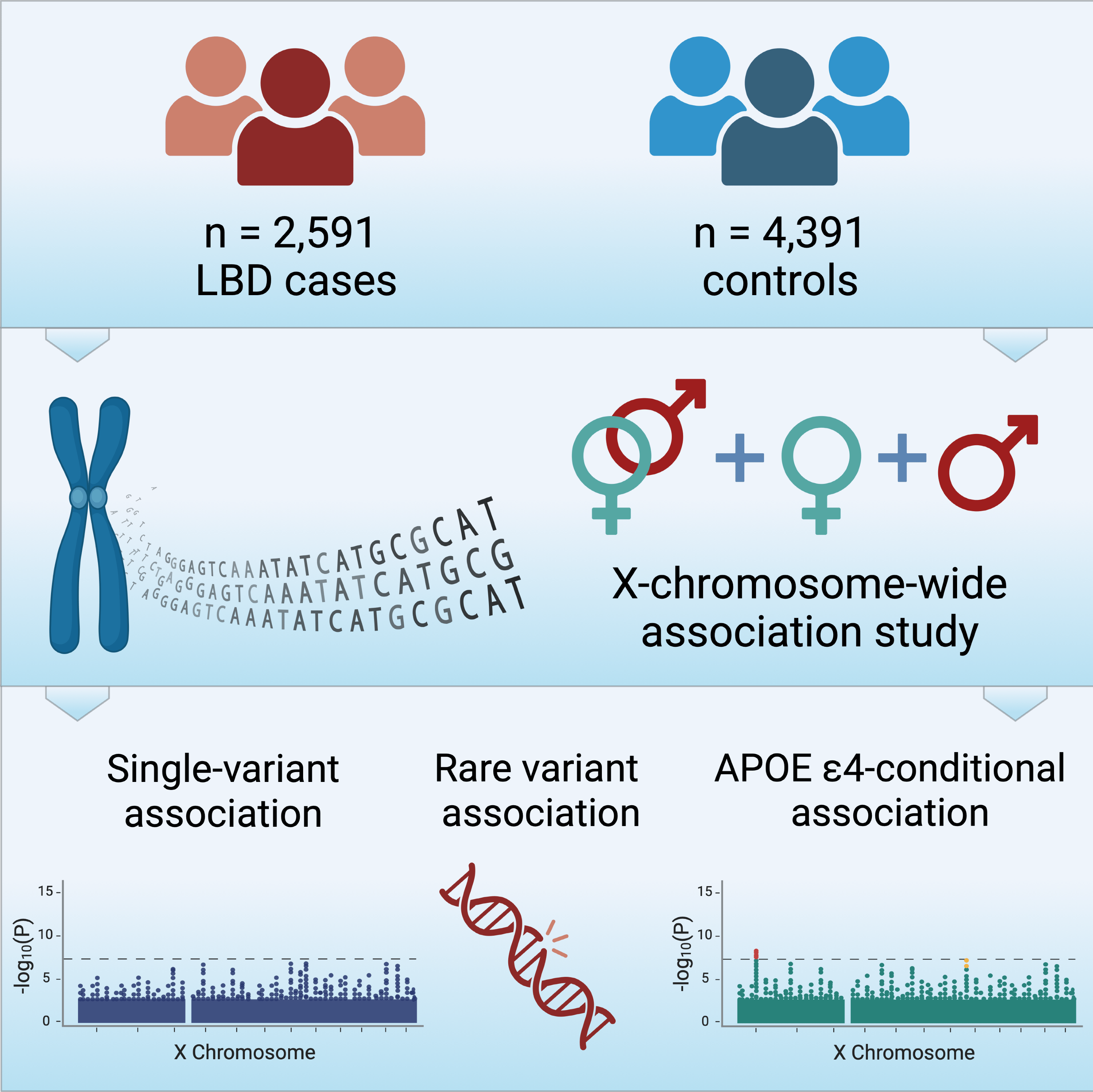
We did not find a significant hit for common and rare variants, but we found a significant hit once we adjusted the analysis for APOEe4. A locus within intron 1 of MAP3K15 was associated with risk for Lewy body dementia only for females. MAP3K15 does not have any previously reported neurodegenerative disease links to the best of our knowledge, but it has been implicated in type 2 diabetes. The gene is a part of a large family that has to do with the MAPK pathway. MAPK pathways have to do with neuroinflammatory responses, neuronal death triggered by alpha-synuclein aggregates, and tau and amyloid precursor protein phosphorylation. Alpha-synuclein aggregates are what make up Lewy body pathology. Tau and amyloid are Alzheimer’s disease pathologies. From studies on Alzheimer’s, we know that the severity of pathology as well as the clinical association of the pathology differs by sex; with females getting hit more once the pathology is severe. This may tie into the females with Lewy body pathology potentially having a higher risk of Alzheimer’s co-pathology compared to males, and Alzheimer’s co-pathology being associated with a higher risk for dementia for females than males with Lewy body pathology.
We also performed a regulome-wide association study to see how this significant variant we found may change the gene expression levels in Lewy body dementia, to have an insight into genetic mechanism. This analysis pointed to ganglionic eminence cells and suggested a role for developmental factors in Lewy body dementia, particularly for females. Ganglionic eminence cells give rise to the basal ganglia, thalamic, olfactory, and majority of cortical interneurons during development. Studies have shown basal forebrain cholinergic neuron loss in Lewy body dementia; basal forebrain cholinergic neuron, and GABAergic interneuron dysfunction were associated with learning and memory impairment in Alzheimer’s disease. Although we did not identify any further significant common or rare variants associated with Lewy body dementia risk, it is still worthwhile to mention there were several sub-significant hits we noted that may come up in future studies.
Overall, our findings hint at sex-specific effects of genetic factors and that changes may start very early in life to eventually lead to Lewy body dementia. The lack of a replication cohort, detailed clinical and pathological information, diversity, and small sample size were important limitations we need to note. The clinical diagnostic criteria for Lewy body dementia will still see more updates, and we may see the definitions change with new promising alpha-synuclein biomarkers alongside Alzheimer’s biomarkers becoming accessible to people. However, we believe our work does show that there is more to genetics than autosomal variants in Lewy body dementia. Our work is just the beginning of efforts looking into the X chromosome in this dementia. There is still much to elucidate in terms of genetic risk and the role of genetic variants in Lewy body dementia, and we cannot emphasize the importance of joining efforts and sharing data on a global scale to better understand and address the needs of the people living with Lewy body dementia.
Follow the Topic
-
npj Parkinson's Disease
This journal publishes original basic science, translational and clinical research related to Parkinson's disease, including anatomy, etiology, genetics, cellular and molecular physiology, neurophysiology, epidemiology and therapeutic development and treatments.

Related Collections
With Collections, you can get published faster and increase your visibility.
The neuroimmune-axis and ageing in Parkinson’s Disease
Publishing Model: Open Access
Deadline: Jul 15, 2026
Cognition - preclinical models, and preclinical unmet need
Publishing Model: Open Access
Deadline: Jul 27, 2026

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in