Behind Enemy Lines: How Cancer Persists by Hiding from our Immune System
Published in Cancer and Anatomy & Physiology
The problem of cancer persistence and recurrence
As a physician specializing in liver cancer, I often sit with patients in the clinic, reviewing scans after treatments. Even when scans show what appears to be a complete response, suggesting the tumor is fully eradicated, I advise my patients to remain hopeful yet vigilant. Our experience has shown that, more often than not, microscopic residual disease persists and, regrettably, leads to recurrence. Such recurrences are especially common in hepatocellular carcinoma (HCC), the most common type of primary liver cancer which is notoriously difficult to cure, and contributes to over 800,000 deaths annually worldwide. Despite advances in treatment, survival rates in HCC have not improved significantly over the past decades. The tendency of HCC to recur is a major reason why we are not able to achieve a sustained cure.
Mechanisms by which macrophages facilitate residual tumor cells to persist
Transarterial chemoembolization (TACE), the most commonly used treatment for unresectable HCC. But it does not lead to sustained cure. The core issue stems from residual tumor cells that survive post-treatment, evade immune detection, and ultimately lead to recurrence. In this study, our main objective was to unravel the mechanisms that allow post-treatment residual cells to persist and to develop strategies that can eliminate them. Technically, studying post-TACE residual HCC in humans has been challenging because the treatment often results in extensive necrosis, leaving only small, scattered areas of viable disease tissue for analysis.
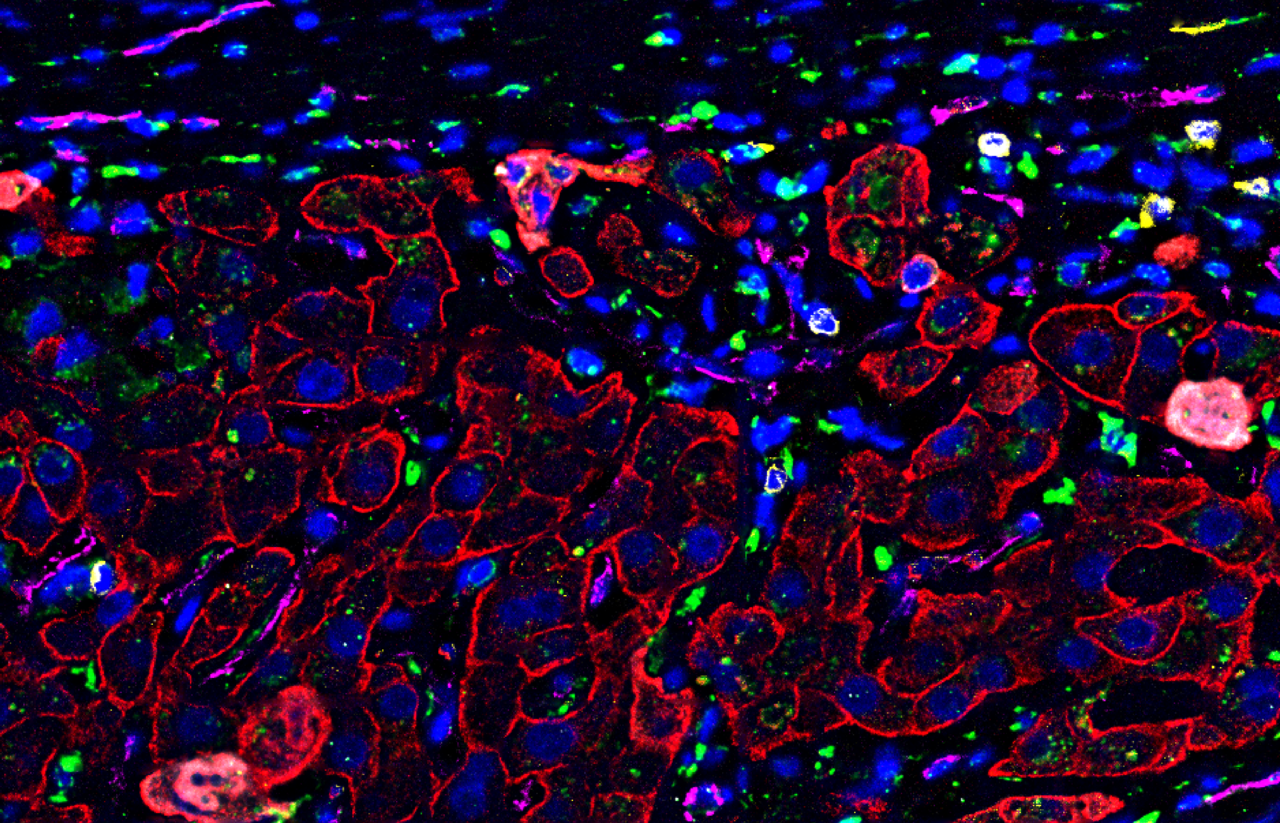
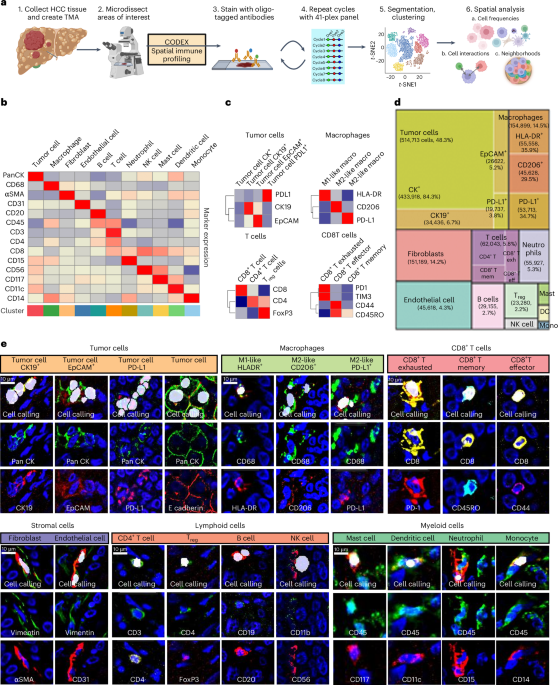
We focused on a cohort of patients who had undergone multiple TACE procedures yet still had residual disease. We knew that the spatial context would be crucial, so we employed cutting-edge technologies that allow us to analyze at a single cell resolution while still preserving the architecture of the tissue. We profiled n=108 samples- 1.07 million cells. Our spatial analysis demonstrated that residual HCC, in contrast to treatment-naïve primary HCC, is organized into distinct neighborhoods within which pro-tumor PDL1+ macrophages shield cancer stem cells from CD8T cell attacks. These stem-cell rich spatial neighborhoods were linked to poor patient outcomes. Additionally, using spatial transcriptomics, we identified a mechanism where these PDL1+ macrophages potentially secrete TGFβ1 to promote the survival of residual cancer stem cells. Thus, our spatial analysis led to the hypothesis that blocking both PDL1 and TGFβ1 could disrupt macrophage-tumor-stem-cell interactions and prevent recurrence.
Developing mouse models to study minimal residual disease (MRD) in HCC
In order to test the above hypothesis we needed mouse models of minimal residual disease (MRD), which refers to a state where no macroscopic disease is detectable, yet hidden or dormant tumor cells persist, eventually causing recurrence. While there are many mouse models to study cancer progression, models which capture the complexities of MRD in solid tumors are rare. Mouse models that effectively simulate MRD need to capture a set of specific characteristics to closely reflect the human condition. These include tumor development in an immunocompetent host to maintain the tumor-immune interactions, tumor regression without any visible disease, and the persistence of microscopic foci of dormant tumor cells that are the direct source of recurrence. To meet these criteria, we employed transgenic mouse models of MYC-driven liver cancer that closely mimic these aspects of MRD. In these models, inactivating the oncogenes led to near-complete tumor regression but microscopic foci of cancer stem cells remained viable. Using these mouse models, we confirmed that Pdl1+ macrophages, through their secretion of Tgfβ1, facilitate the persistence of stem-like tumor cells—a mechanism of HCC dormancy conserved across species.
Therapeutic strategy to prevent recurrence from MRD in mouse HCC
Our next set of in vivo experiments were exciting since they confirmed our hypothesis. We demonstrated that dual inhibition of Pdl and the Tgfβ pathway, and not their individual blockade, was highly effective in preventing HCC recurrence from MRD in our mouse models. We found that the combined treatment not only blocked macrophages from shielding the dormant tumor cells but also activated CD8T cells to eradicate them. Additionally, we validated these results using another model of chemotherapy-resistant HCC. Thus, our approach holds significant promise for improving outcomes in HCC by targeting the microenvironment that supports cancer dormancy and recurrence.
Implications of our findings in the management of HCC
In summary, our use of advanced single-cell spatial mapping has uncovered critical interactions between macrophages and cancer stem cells in post-TACE residual HCC which facilitated the residual cancer cells to evade detection by CD8T cells. The use of comprehensive single-cell spatial analysis provided us with mechanistic insights that would not have been accessible if the tissue had been dissociated for other assays like flow cytometry or single-cell sequencing. Furthermore, our analysis of human samples pinpointed a targeted approach that could significantly reduce recurrence and improve patient outcomes.
Several adjuvant therapies for HCC are currently in development, though none have yet received approval, and the optimal timing and modalities of treatment are yet to be determined. Our findings endorse a brief combined blockade of TGFβ1 and PDL1 as an effective strategy to prevent recurrence following TACE. Moreover, this strategy might also be applicable to managing other types of post-treatment MRD. While this combination has yielded inconsistent results in other cancers and shown potential toxicity with prolonged use, our research indicates that short-term application specifically tailored for MRD contexts can potentially effectively prevent recurrence.
On a personal note, as I continue to monitor patients with HCC under surveillance in my clinic, balancing hope with caution, our research brings a wave of optimism. I am optimistic the clinical practice will change from just monitoring for HCC recurrence to proactively preventing it with adjuvant therapies. These advancements promise to disrupt the cycle of surveillance and anxiety our patients feel, paving the way toward a real, sustained cure.
Follow the Topic
-
Nature Cancer

This journal aims to provide a unique forum through which the cancer community will learn about the latest, most significant cancer-related advances across the life, physical, applied and social sciences.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in