Crafting 'Smarter' Drug Testing to Facilitate Harm Reduction
Published in Chemistry, Biomedical Research, and General & Internal Medicine

Every investigation has a story!
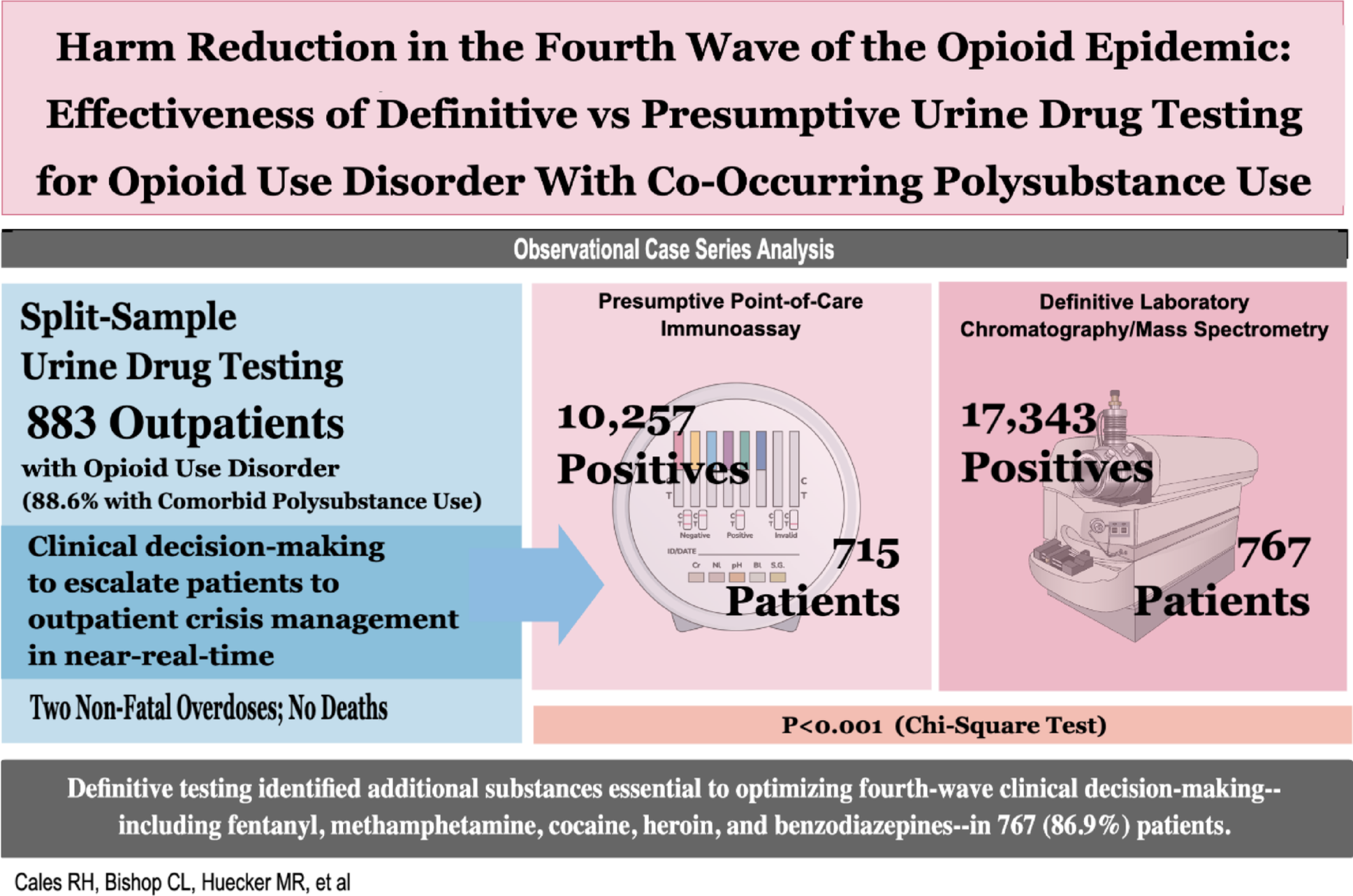
Herein, we detail the unanticipated yet fortuitous events leading to our recent Harm Reduction Journal publication, titled “Harm Reduction in the Fourth Wave of the Opioid Epidemic: A Case Series Investigation of the Effectiveness of Definitive vs Presumptive Urine Drug Testing for Opioid Use Disorder with Co-Occurring Polysubstance Use.” 1
INTRODUCTION
Our inquiry presents the first peer-reviewed investigation to evaluate evidence-based effectiveness, medical necessity, and expense of 'smarter' drug testing2—using near-real-time mass spectrometry rather than less costly immunoassay testing to guide both clinical decision-making and harm reduction in substance use disorder patients with co-occurring polysubstance use disorder in a real-world, outpatient, buprenorphine MOUD (medication for opioid use disorder) setting.
Acknowledging that an illustration can provide an attractive alternative to a 2,500-word manuscript, we offer the following:
.png)
BACKGROUND
When we established our clinic network a decade ago, we initially adopted point-of-care immunoassay as our testing modality. Very quickly, however, we encountered two concerning trends. First, nearly two-thirds of point-of-care immunoassay samples revealed one or more substances requiring laboratory confirmation using mass spectrometry. Second, as part of the confirmation process, the laboratory using mass spectrometry to process our specimens reported finding a disturbing number of additional, unsuspected substances—which they detected as part of their routine, in-house quality assurance processes—in our test samples that a) we had not ordered, and b) represented drugs most often found in autopsies of fatal overdoses (ie, fentanyl, cocaine, amphetamine, methamphetamine, and benzodiazepines).
Although the available medical literature initially provided limited insight, we found several resources that pointed to the need for exploratory research on using point-of-care immunoassay vs laboratory/mass spectrometry technology for clinical management of substance use disorder patients.
- ASAM: A 2013 white paper introducing the concept of 'smarter' drug testing, followed in 2017 by a more detailed consensus statement on the topic.2
- Barthwell et al: Two publications (cited in manuscript), including a literature review, underscoring the importance of specifying laboratory testing as the primary methodology to minimize both false positives and false negatives.
- Five additional publications (cited in manuscript) spanning the last decade detailing the experiences of Millenium Health’s reference laboratory, which mirror our findings of significant, concerning discovery of unordered and unexpected substances detected in urine samples.
- Nora Volkow’s NIDA editorial perspective in 2023 in the New England Journal of Medicine calling for evaluation of the feasibility of expanding drug testing to include laboratory testing to facilitate harm reduction in real-world clinical settings.3
To the best of our knowledge, our investigation is the first peer-reviewed effort to address the potential for leveraging near-real-time laboratory testing to expand the realm of harm reduction for substance use disorders in a real-world, outpatient clinical setting.
INVESTIGATION
Our case series included all opioid use disorder patients, most of whom exhibited co-occurring polysubstance use, treated with buprenorphine MOUD for one year in a single outpatient clinic. Interventions entailed head-to-head, split-sample urine drug testing that compared definitive laboratory chromatography/mass spectrometry testing to less-costly presumptive point-of-care immunoassay testing, which is more susceptible to false-positive and false-negative results. Outcomes included return to use during treatment, morbidity, and mortality.
Urine Drug Testing
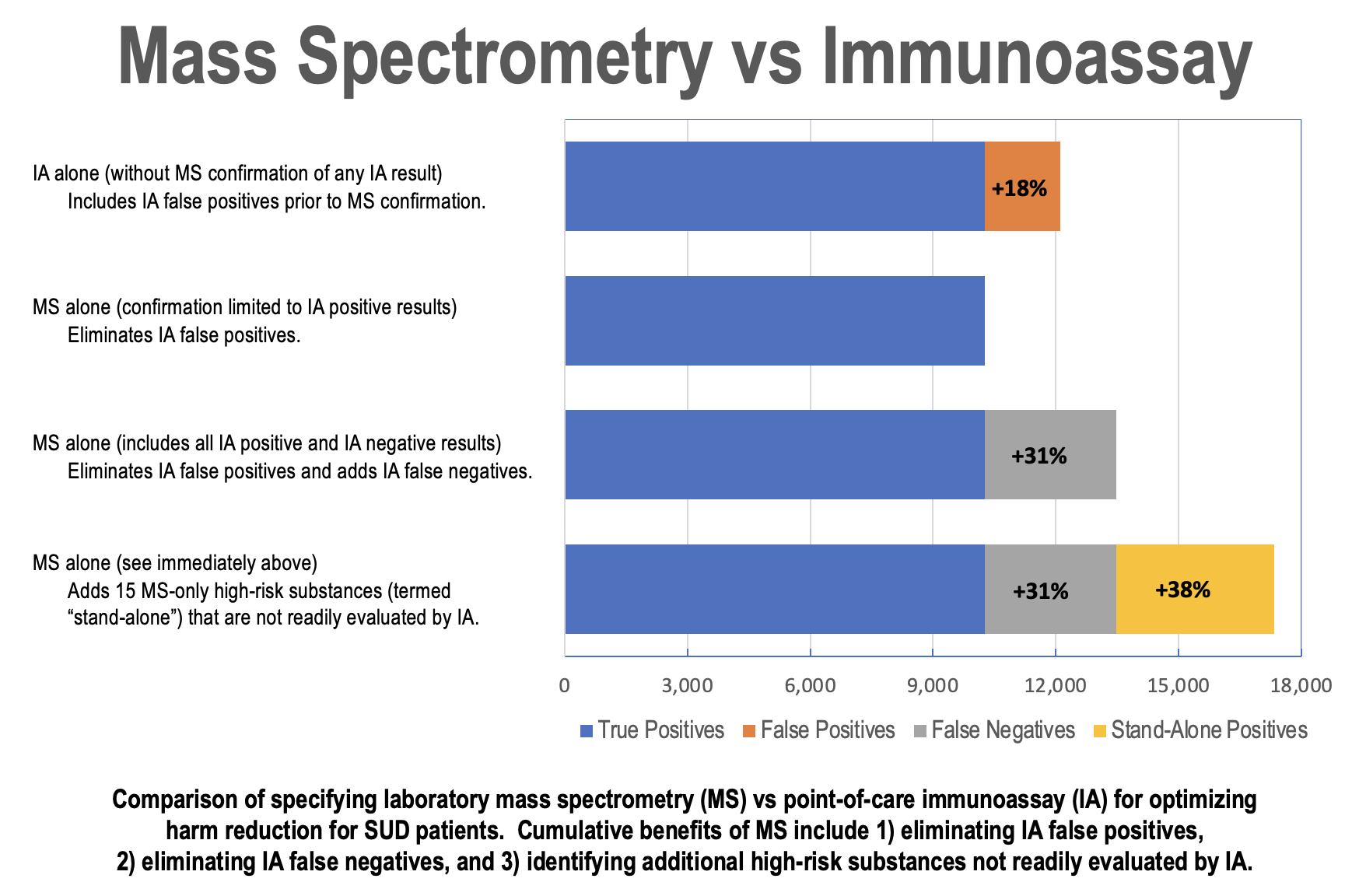
With regard to the superiority of laboratory mass spectrometry vs point-of-care immunoassay , our investigation is one of the first to report effectiveness of both the incidence and clinical relevance of using MS in a real-world, community clinic setting, not merely by eliminating false positives and false negatives but also by further leveraging mass spectrometry technology to identify other high-risk substances critical to optimizing harm reduction.
Harm Reduction
Although the term “harm reduction” most often appears in the context of substance use disorders and intravenous drug use, the public health community has long used the term to characterize a broad spectrum of preventive considerations, as illustrated by the following:

In this regard, our investigation is one of the first to respond to NIDA’s exhortation3 for clinicians to contribute to the ever-expanding scope of drug testing to include both real-time immunoassay test strips and near-real-time laboratory mass spectrometry testing to facilitate harm reduction.
Although some of our findings regarding the sensitivity and specificity of presumptive testing are neither new nor unexpected, we believe that our overall findings and resulting conclusions are unique in that they are the first to be reported a) in a single cohort of OUD patients with co-occurring polysubstance use employing split-sample presumptive vs. definitive testing and b) in the context of medical decision-making based on definitive UDT to facilitate harm reduction by guiding and escalating care in near real-time.
TAKEAWAYS
Our investigation offers three takeaways of particular relevance to real-world clinical practice:
- Although point-of-care immunoassay may suffice for population-based screening (initial detection and referral), medical decision-making (diagnosis and management) for MOUD is better served by near-real-time definitive laboratory testing.
- Our 'smarter' drug testing experience demonstrates that using non-quantitative, near-real-time testing for MOUD patients virtually eliminates the need for point-of-care testing—which requires confirmatory laboratory testing for more than half (57.6%) of all point-of-care tests due to one or more positive presumptive findings—yet costs only $10 more per patient encounter.
- These findings have facilitated the opportunity to integrate MOUD with harm reduction by refining 'smarter' definitive laboratory testing protocols to detect emerging and novel substances, including but not limited to kratom, xylazine, carfentanil, dexmedetomidine, tianeptine, levamisole, bromazolam, and nitazenes.
Hopefully, our exploratory findings will be serve to inform more robust additional research.
REFERENCES
- Cales RH, Bishop CL, Huecker MR, et al. Harm reduction in the fourth wave of the opioid epidemic: A case series investigation of the effectiveness of definitive vs presumptive urine drug testing for opioid use disorder with co-occurring polysubstance use. Harm Reduct J. 22, 187 (2025). https://doi.org/10.1186/s12954-025-01335-4
- Jarvis M, Williams J, Hurford M, et al. Appropriate use of drug testing in clinical addiction medicine. J Addict Med. 2017;11(3):163–173.
- Volkow ND, Califf RM, Sokolowska M, Tabak LA, Compton WM. (2023). Testing for fentanyl—Urgent need for practice relevant and public health research. NEJM. 388(224):2214-2217.
Physician healthcare advocate with five decades of experience both in providing care for individual patients and in developing, managing and evaluating statewide healthcare systems throughout the United States.
Specializing in internal medicine, emergency medicine, and addiction medicine, I have published multiple peer-reviewed investigations and edited multiple books on EMS systems (emergency medical services), trauma care systems (trauma centers), and addiction medicine (substance use disorders).
Focusing on developing and managing cutting-edge information technology—encompassing individual patients to entire populations—to create and maintain intuitive electronic health record systems that facilitate transforming chaotic data into readily actionable information for both individual patients and global public health.
Follow the Topic
-
Harm Reduction Journal
This journal publishes research and commentary on approaches diminishing the harm of stigmatization, marginalization and criminalization of public health, human rights and social justice issues, as well as rebuking the de facto criminalization of marginalized and stigmatized communities.

Related Collections
With Collections, you can get published faster and increase your visibility.
The Enhanced Games: Human Enhancement, Risk, and Harm Reduction in a Post-Doping Era
Debates about performance-enhancing substances in sport have historically been framed through prohibition, anti-doping enforcement, and ideals of fairness, natural ability, and sport integrity. The proposed Enhanced Games – an international sporting event that explicitly permits the use of performance-enhancing substances – have been presented as a profound rupture in how sport, medicine, and society understand human limits, bodily risk, and enhancement. This collection asks what it means to govern, reduce harm, and protect wellbeing in a world where the use of performance-enhancement substances is increasingly visible, normalised, and commercialised.
The Enhanced Games position themselves as rejecting prohibition, reframing enhancement as positive when transparent and regulated, and describe it as technologically inevitable. In doing so, the Games propose a departure from paternalistic-type interventions in favour of autonomy and science. However, the goals of the Enhanced Games stretch far beyond the sporting arena into the supplement and pharmaceutical industries, sparking concerns regarding competing and conflicting interests. Their scale, visibility, and commercial profile have drawn significant public attention, making questions about governance, enhancement, health, fairness, and harm increasingly urgent to address.
Importantly, this collection does not advocate for or against the Enhanced Games. Instead, it aims to provide a forum for scholarly discussion of the ethical, clinical, regulatory, and social questions raised by this proposal. Given the limited empirical literature currently examining such models of openly permitted enhancement, contributions both supporting and critically challenging this idea are particularly needed. This Collection is explicitly dedicated to examining the Enhanced Games as a social, ethical, public health, and harm reduction phenomenon.
Beyond the existence of human enhancement, the Enhanced Games themselves raise urgent questions:
- Could an openly permitted and regulated model of performance enhancement reduce or mitigate harms associated with the current prohibition of enhancement drugs in sport?
- What are the strongest arguments against such an approach, and how do these concerns compare with the potential benefits claimed by proponents?
- Who bears responsibility for risk in environments where pharmacological enhancement is permitted?
- What does autonomy look like within the Enhanced Games model?
- What constitutes informed consent in high-stakes, financially sponsored performance contexts?
- Can harm reduction meaningfully coexist with elite competition and commercial sport promoted as spectacle?
- Are the vast monetary rewards offered the Enhanced Games for athletes that break ‘world records’ a coercive offer?
- Are there differences between public perceptions of the Games and the realities of athlete participation, and how might both shape decision-making among athletes and spectators?
- Are athletes vulnerable within the Enhanced Games model?
- What lessons might this model offer for broader enhancement practices beyond sport?
The Harm Reduction Journal invites interdisciplinary contributions that critically engage with the Enhanced Games, situating them within wider enhancement cultures, drug use practices, regulatory systems, and harm reduction frameworks. The legitimacy of the Enhanced Games as an alternative model for harm reduction remains an open question. Lived-living experience perspectives on enhancement and risk are specifically encouraged.
This Collection aims to provide the first dedicated harm reduction–focused scholarly examination of the Enhanced Games. The Editors seek to promote evidence-based analysis and discussion of policy, sport governance, and public health responses to emerging enhancement models.
Scope of the Special Issue
We welcome empirical, theoretical, policy, and commentary papers addressing topics including, but not limited to:
1. Enhanced Games–Embedded Research and Case Studies
Empirical papers drawing directly on the Enhanced Games, affiliated teams, athletes, or operational settings, including, where ethically appropriate and critically engaged:
- Biomedical, performance, and health monitoring data from Enhanced Games athletes
- Case studies of elite athletes using enhancement drugs within enhancement-permissive environments
- Governance, safety, and medical oversight models implemented by the Enhanced Games
- Ethical and operational challenges encountered in practice
2. Comparative Studies, Trials, and Harm Analysis
Research examining empirical evidence that may support or challenge the implementation of the Enhanced Games, including quantitative, qualitative, mixed-methods, and trial-based studies that compare:
- Enhanced Games athletes using enhancement drugs vs elite athletes operating under prohibition-based regimes
- Elite athletes using enhancement drugs vs non-athletes using similar substances
- Consumers vs non-consumers in comparable populations (e.g., fitness, strength, or aesthetic domains)
3. Commentary, Policy, and Lived-Living Experience
Analytical and reflective contributions examining:
- Ethical, legal, and public health implications of the Enhanced Games
- Athlete autonomy, consent, coercion, and commercialisation
- Lived and living experience of athletes and others who use enhancement drugs
- Perspectives from clinicians, harm reduction workers, regulators, and policymakers
- Implications for future sport governance, drug policy, and harm reduction frameworks
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this collection undergo the journal’s standard peer review process. Where necessary, Guest Editors will ensure peer-review is provided by those unaffiliated with the Enhanced Games in any way and will ensure diversity is strongly considered with regards to gender, ethnicity, geography and lived/living experience. All manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (APC). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit Harm Reduction Journal's Fees and Funding page, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Dec 16, 2026
Repairable damage: harm reduction and US policy
Recent shifts in US policy and the approach to public health have placed renewed pressure on communities that already face significant health and social challenges. Policy decisions increasingly prioritize criminalization or abstinence-based strategies over interventions that have been consistently shown to reduce harm. These choices reflect a broader trend of sidelining empirical evidence, with real-world consequences for public health.
As a result, morbidity and mortality have increased among people who use drugs, experience homelessness, or who are involved in the US criminal justice system. Rates of preventable illness and infectious disease are also rising. Rhetoric and stigma further undermine public trust and discourage engagement with health services, disproportionately affecting marginalized populations.
Harm Reduction Journal has commissioned a collection of articles to highlight how evidence-based harm reduction strategies – grounded in science, dignity and practical outcomes – can inform more effective, humane public health responses.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being, SDG 5, Gender Equality, SDG 10, Reduced Inequalities, and SDG 16, Peace, Justice and Strong Institutions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Aug 18, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in