Cyberbullying and Depression: What National Data Reveal About Bangladeshi Adolescent Girls
Published in Social Sciences, General & Internal Medicine, and Behavioural Sciences & Psychology
Cyberbullying has become part of everyday life for many young people, but in Bangladesh, we still know surprisingly little about how it affects female adolescents’ mental health at the national level. This paper grew out of a simple but worrying question: what does cyberbullying really mean for the mental well-being of Bangladeshi female adolescents once you look beyond small, urban, or school‑based samples?
Why we did this study
In recent years, reports of online harassment, digital abuse, and cyberbullying against Bangladeshi girls and young women have grown rapidly, especially on social media platforms like Facebook and messaging apps. Local studies and NGO reports were signalling high levels of online violence, but most of this evidence came from specific schools, colleges, or urban groups, and could not tell us what was happening across the whole country. At the same time, global research was increasingly clear that cyberbullying is not just “online drama,” it is linked to major depressive disorder (MDD), self‑harm, and other serious mental health problems.
Bangladesh now has a national strategy for adolescent health that explicitly recognizes adolescent girls as a vulnerable group and calls for protecting them from violence, harassment, and mental health risks. Yet, nationally representative data on cyberbullying and depression among female adolescents were missing, which meant policymakers were essentially working in the dark. That gap was our starting point.
The opportunity: a national adolescent survey
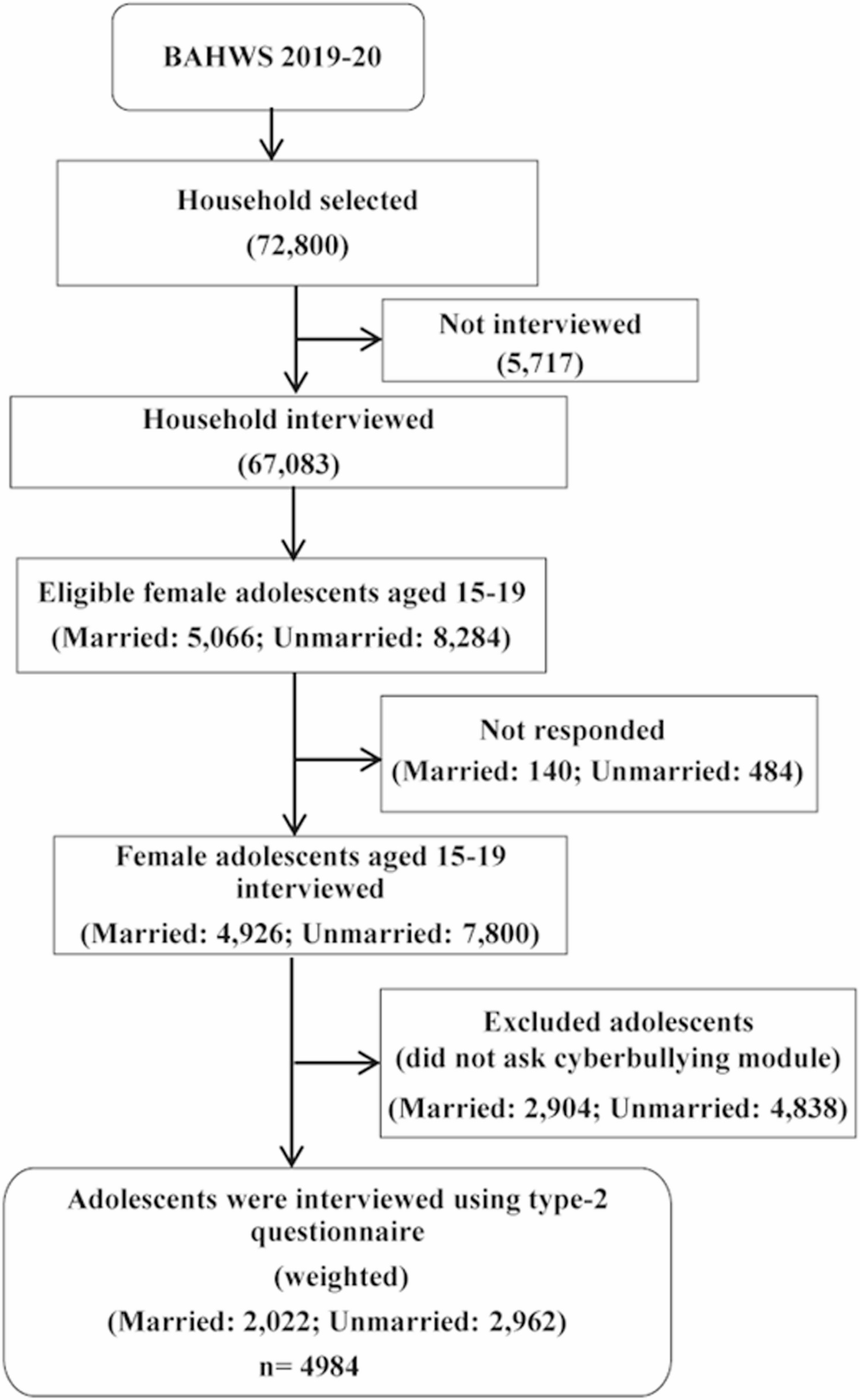
The turning point came with the Bangladesh Adolescent Health and Wellbeing Survey (BAHWS) 2019–20, a large national survey covering adolescents aged 15–19 years from all eight divisions, urban and rural areas. BAHWS included a question on cyberbullying (“Has anyone used mobile/internet to bother/harass you at least once in the last 12 months?”) and the full PHQ‑9 scale to screen for major depressive disorder.
For us, this was a rare opportunity: in one dataset, we could see who was being bullied online, how often, and how that related to their mental health, while also taking into account social and economic background, education, marital status, and region. We focused on female adolescents because evidence consistently shows they are more likely to experience cyberbullying and its psychological consequences than boys, and because BAHWS only included married girls on the female side, not the male side, which would make direct sex comparisons tricky.
How we approached the analysis
We worked with data from 4,984 female adolescents aged 15–19 years who answered the cyberbullying question and completed the PHQ‑9. The sample was nationally representative: about 59% were never‑married, 41% ever‑married, most lived in rural areas, and there was good coverage across all divisions. We defined major depressive disorder as a PHQ‑9 score of 10 or more, a widely used threshold in adolescent mental health research, and the scale showed good internal consistency in this sample (Cronbach’s alpha 0.80).
Cyberbullying exposure was captured in two steps: first, whether the adolescent had been harassed via mobile or internet in the past 12 months, and second, how often this had happened (once or twice, two to four times, or five or more times). We began with descriptive analyses and chi‑square tests to explore how common cyberbullying and MDD were across different subgroups and then used multiple logistic regression to estimate the association between cyberbullying and MDD while adjusting for age, marital status, schooling, employment, wealth, mobile phone ownership, Facebook use, residence, and division.
What we found
Several findings stood out clearly. First, major depressive disorder is not rare in this group. Overall, 12.4% of female adolescents met the PHQ‑9 threshold for MDD, with higher prevalence among 19‑year‑olds, ever‑married girls, those with fewer years of schooling, and those in some divisions, such as Mymensingh. This means roughly one in eight girls in late adolescence is living with depressive symptoms severe enough to interfere with daily life.
Second, cyberbullying is common but unevenly distributed. About 8–12% of girls (depending on the definition used in the paper sections) reported that someone had used a mobile or internet to bother or harass them in the last 12 months, with variation by region and other factors. For example, Barisal, Rangpur, and Mymensingh showed some of the highest reported levels of cyberbullying, while Sylhet had the lowest. Many girls were bullied by unknown people online, but friends, classmates, neighbours, and even husbands or in‑laws (for ever‑married adolescents) also appeared as perpetrators.
Third, and most importantly, there was a strong association between cyberbullying and major depressive disorder. Among girls who had not experienced cyberbullying, about 10–11% had MDD, while among those who had been cyberbullied, around 32% had MDD. In other words, nearly one in three cyberbullied girls was living with major depressive symptoms.
When we adjusted for other factors in the logistic regression model, adolescents who experienced any cyberbullying in the past 12 months were almost four times more likely to have MDD than those who did not (AOR 3.97, 95% CI 3.12–5.05). We also saw a clear dose-response pattern: the more frequently a girl was cyberbullied, the higher her chance of having MDD. Those bullied once or twice had an elevated risk; those bullied five or more times had the highest burden of depression.
To visualize this for a non‑technical audience, we used bar charts: one set showing MDD prevalence by cyberbullying status (no vs yes), and another showing MDD rising stepwise as cyberbullying frequency increased. Even without statistical training, the story in those figures is obvious.
What surprised us
Going into the study, we expected cyberbullying to be associated with depression, based on international evidence, but the strength of the association and the dose–response pattern in a nationally representative Bangladeshi sample were still striking. It was also sobering to see how often the perpetrator was an unknown person online, which hints at the challenge of regulating digital spaces and the sense of helplessness victims may feel.
Another important element was the social and legal context. Bangladesh has several laws that can cover forms of cyberbullying, the ICT Act, Pornography Control Act, and, most recently, the Cyber Security Act 2023, but “cyberbullying” is not explicitly named, and awareness of rights and reporting channels remains low. At the same time, strong gender norms, concerns about “honour,” and fear of stigma mean that many girls and families hesitate to report online abuse, even when legal and police mechanisms exist.
What this means in practice
For us, the key message is that cyberbullying is not a niche problem confined to a few elite schools in Dhaka (the capital); it is a nationwide issue that is measurably linked to serious mental health problems among female adolescents. The finding that risk increases with repeated cyberbullying suggests that early recognition and prompt reporting could be critical in preventing worsening depression.
The paper argues for several practical steps:
-
Build clear, accessible reporting mechanisms in schools and communities, so girls know where to turn when they are harassed online.
-
Train teachers, parents, and health workers to recognize signs of cyberbullying and depression and to respond in a supportive, non‑judgmental way.
-
Integrate digital safety and mental health literacy into school curricula and youth programs, with a special focus on girls’ experiences online.
-
Strengthen and publicize existing legal protections and helplines, while ensuring that responses are victim‑centered and do not further stigmatize girls.
-
Expand adolescent‑friendly mental health services, particularly in regions with high cyberbullying and MDD burden.
Looking ahead
This study is, to our knowledge, the first to use nationally representative data to quantify the link between cyberbullying and major depressive disorder among Bangladeshi female adolescents. It confirms that cyberbullying is not just an online inconvenience but a serious public health issue with clear mental health consequences.
At the same time, our work has limitations: cyberbullying was measured with a single survey question rather than a detailed, validated scale, the design is cross‑sectional, and we only included girls aged 15–19, leaving out younger adolescents. Future research can build on this by using longitudinal designs, richer measures of online experiences, and including both sexes and younger age groups.
For now, we hope this paper helps push cyberbullying and adolescent mental health further up the policy agenda in Bangladesh, and supports those already working to make digital spaces safer for girls.
Follow the Topic
-
BMC Psychiatry
This is an open access, peer-reviewed journal that encompasses a wide range of topics, including psychopharmacology, psychotherapy, and psychosocial approaches to psychiatric disorders, as well as genetics, pathophysiology, and epidemiology research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Sleep problems and psychiatric disorders
The intricate relationship between sleep problems and psychiatric disorders presents a fertile ground for exploration and understanding. Disruptions in sleep patterns and circadian function are not merely symptoms; they often serve as pivotal markers for a range of mental health issues, including depression, bipolar disorder, anxiety, and schizophrenia.
Sleep disturbances can exacerbate existing psychiatric disorders, complicating clinical presentations and treatment responses. Conversely, managing sleep and circadian problems can result in significant improvements in psychiatric outcomes, underlining the need for an integrative approach in both research and clinical practice. Recent studies have elucidated the biological and physiological mechanisms linking sleep disruption to mood dysregulation, revealing insights into neurotransmitter pathways and hormonal imbalances.
In this context, we invite researchers to contribute original research and review papers that will enhance our understanding of sleep problems and their intricate relationship with psychiatric disorders. Topics of interest include but are not limited to:
- The role of circadian rhythms in psychiatric disorders
- Sleep disorders as predictors of mood disorders
- Treatment efficacy of CBT-I or chronotherapy in psychiatric populations
- Bi-directional effects of sleep and mental health
- Neurobiological mechanisms linking sleep and mood
- Impact of sleep hygiene interventions on mental health
- Sleep architecture in severe psychiatric conditions
- Longitudinal studies on sleep patterns and psychiatric outcomes
- Prevention and early-intervention studies targeting sleep and circadian function
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer-review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 3: Good Health and Well-being.
Publishing Model: Open Access
Deadline: Feb 01, 2027
Alcohol use and psychiatric disorders
BMC Psychiatry is calling for submissions to our Collection on Alcohol use and psychiatric disorders. Alcohol use remains a leading contributor to global morbidity and mortality and is frequently associated with a wide range of psychiatric disorders, complicating diagnosis, treatment, and long-term outcomes. The co-occurrence of alcohol-related problems and psychiatric conditions poses significant challenges for patients, clinicians, and health systems alike.
This Collection aims to advance understanding of the relationship between alcohol use and psychiatric disorders across the lifespan. We welcome contributions that address underlying mechanisms, clinical presentations, and integrated approaches to assessment and treatment in both acute and long-term care settings.
Topics of interest include, but are not limited to:
- Epidemiology and patterns of comorbidity between alcohol use disorder and psychiatric diagnoses
- Alcohol use disorder in the context of major depressive disorder, anxiety disorders, bipolar disorder, schizophrenia, and trauma-related disorders
- Diagnostic challenges, including symptom overlap, masking effects, and differential diagnosis
- Neurobiological and genetic factors contributing to co-occurring alcohol use and psychiatric disorders
- Pharmacological and psychosocial treatment strategies, including relapse prevention and management of withdrawal
- The impact of alcohol use on treatment response, adherence, and prognosis in psychiatric populations
- Suicide risk, self-harm, and behavioral dysregulation associated with alcohol use and psychiatric illness
- Developmental and lifespan perspectives on alcohol use and psychiatric comorbidity, including adolescence and young adulthood
- Health disparities, stigma, and barriers to accessing integrated addiction and psychiatric care
We invite original research exploring how alcohol use interacts with psychiatric disorders and how care can be optimized for affected individuals. By integrating evidence from clinical practice, epidemiology, and health services research, this Collection seeks to inform effective, compassionate, and coordinated models of care.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 3: Good Health and Well-Being.
Publishing Model: Open Access
Deadline: Dec 11, 2026
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in