From a remarkable response to anti-PD-1 rechallenge to a cancer-free assisted dying
Published in Cancer and Immunology
Fumarate hydratase-mutated/deficient papillary renal cell carcinoma (pRCC) is a unique kidney cancer subtype marked by mutations in the fumarate hydratase (FH) gene, an enzyme in the Krebs cycle that converts fumarate into malate to keep the life-powering cycle going. A deficit in this enzyme leads to fumarate buildup inside the cells, which has several consequences. Excess fumarate causes metabolic disruption, damage to subcellular components, dysregulation of the cell cycle, epigenetic modifications, and the stabilization of the hypoxia-inducible factor (HIF) pathway, all of which contribute to cancer development. Kidney cells are particularly predisposed to tumorigenesis, although virtually all the cells from a patient bearing an FH deficiency may experience fumarate excess and its effects. Within the tumor microenvironment, an activated HIF pathway leads antitumor T cells to exhaustion and to upregulate inhibitory checkpoint molecules in their surface, such as PD-1. Thus, immunotherapy with anti-PD-1 holds huge promise by restoring T cells’ functions, even under the pressure of such a toxic milieu. It sounds nearly ideal in theory; however, anti-PD-1 was not available when my patient was initially diagnosed in 2010, and when it eventually became an option, it was prematurely discontinued as he was thought to be a non-responder when, in fact, he was a responder. When restored, anti-PD-1 turned him into a cancer-free patient… at a cost.
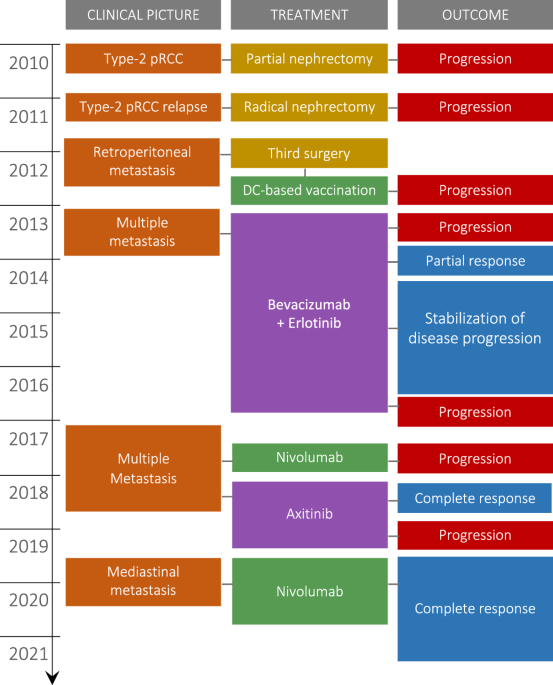
Behind this paper, there was a special human being who battled and defeated cancer as a true warrior. For more than a decade, living with and without cancer, he outlived his relatives who, within months after diagnosis, succumbed to the running-in-the-family FH-mutated pRCC. We first met in 2012 in Sao Paulo, Brazil, and I noticed immediately that he was a unique patient. In Colombia, his home country, he was offered a last surgery to remove local metastasis after undergoing partial and radical nephrectomies, but nothing else was offered after that. He was eager to live a little more, and knowing the prognosis of his relatives, he was willing and curious to try experimental protocols. We offered him a cancer vaccine protocol that was running at my lab at the time. To formulate the vaccine, we needed tissue from his tumor. His surgery in Colombia was scheduled for August 21st; I remember it vividly. Coincidentally, it was the same day my husband in Brazil was having a partial nephrectomy due to a kidney tumor and possibly getting into the same cancer vaccine protocol. It took an army of colleagues, friends, and family to get his tumor and my husband’s tumor delivered to our lab in Sao Paulo, processed, and stored for upcoming vaccine regimens. He took four doses, but the vaccine might not have worked as we expected. From the samples we collected to monitor his response, we observed a clear break of suppression and anergy in his immune system after three doses, but the tumors were back and worse. We always suspected a pseudoprogression*, but there wasn’t any means to confirm it. Shortly after, we were aware of a clinical trial for him at the NCI – NIH. He went to Bethesda, where his FH mutation was confirmed, and even though he couldn’t enroll in the clinical trial, he was recommended to start on erlotinib plus bevacizumab. Both drugs gave him almost three years of partial response and stabilization of disease progression; the tumor remained dormant in equilibrium with the immune system. But eventually, the tumor pressure outweighed the antitumor immune response, and clinically detectable lesions reappeared.
After that, he was recommended many options, including other TKIs and anti-PD-1. Wanting to avoid adverse events, he opted for anti-PD-1, but after three months, the lesions were apparently worse than before. He was then switched to axitinib and off-label metformin, and by his next scan, 3 months later, he had achieved a spectacular complete response. But then, soon after, while on axitinib, new lesions appeared in a completely new organ, the lungs. He reached back a last time for guidance and, based on a possible second occurrence of pseudoprogression*, one after the cancer vaccine and another during his first anti-PD-1 exposure, we recommended an anti-PD-1 rechallenge. Rapidly, he achieved a complete response again, but this time, it was a sustained response accompanied by high eosinophil blood counts. The origin of eosinophilia was thoroughly investigated and finally granted as an immune-related adverse event to anti-PD-1 and also as a possible biomarker of anti-PD-1 response. However, considering the potential onset of eosinophilia-related issues, anti-PD-1 was discontinued, and prednisone was given to bring eosinophil counts back to normal. He never resumed anti-PD-1, but he held his cancer-free status even without it. But this journey came with a very high cost: permanent and unmanageable adverse events that had a significant impact on his quality of life. Eventually, he opted for assisted dying.
His passing was shocking, and it was the reason why we couldn’t finish his 10-year follow-up before. How come cancer-free patients are opting for assisted dying? I could have rewritten the paper again in different words, but instead, I wanted to take this "behind of the paper" opportunity to give him a voice. After all, it was his wish to share his story with the world in an attempt to help others like him. Our cancer patients deserve more and global access to immunotherapy, deserve pseudoprogression* to be figured out by radiologists/oncologists, deserve tailored approaches for tumor dormancy, deserve better biomarkers of response and toxicity, and deserve us to care more, beyond immunotherapy, about the quality of life of our cancer-free patients. We have achieved remarkable progress; however, it is time that cancer treatments cease to be more detrimental than the disease itself.
*Psedoprogression is when existing tumors appear bigger in follow-up scans, and new lesions can also be seen. When biopsied, those lesions turn out to be inflammatory infiltrates rather than tumor tissue. When imaged after a month or so, they are completely gone. They look like cancer progression, but they are not.
References:
Follow the Topic
-
npj Precision Oncology
An international, peer-reviewed journal committed to publishing cutting-edge scientific research in all aspects of precision oncology from basic science to translational applications to clinical medicine.

Ask the Editor – Inflammation, Metastasis, Cancer Microenvironment and Tumour Immunology
Got a question for the editor about inflammation, metastasis, or tumour immunology? Ask it here!
Continue reading announcementRelated Collections
With Collections, you can get published faster and increase your visibility.
Minimal Residual Disease and Circulating Tumor DNA Dynamics in Personalized Cancer Treatment
Publishing Model: Open Access
Deadline: Mar 12, 2027
Genomic Instability
Publishing Model: Open Access
Deadline: Jun 24, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in