Immunotherapy in Myelodysplastic Neoplasms
Published in Cancer, Biomedical Research, and Pharmacy & Pharmacology

What is Immunotherapy?
Immunotherapy harnesses our immune system to detect and attack cancer cells. T cells, a major component of the immune system, recognize abnormal proteins on the surface of the body’s cells when cancer starts to develop. T cells detect and kill these abnormal cells and eliminate cancer before it progresses. Therefore, the immune system is critical in cancer surveillance and prevention.
However, cancer cells frequently circumvent T-cell surveillance. They do so through the interaction between programmed cell death 1 (PD-1) on the surface of T cells and programmed cell death-ligand 1 (PD-L1) on cancer cells. When PD-1 binds to PD-L1, the interaction sends a suppressive signal to T cells, which prevents the T cell from being activated, consequently allowing the cancer cell to survive. Similarly, cytotoxic T-lymphocyte-associated protein 4 (CTLA4) on T cells binds to B7 on MDS cells, which stifles T cell activation and enables cancer cells to evade the immune system.
Naturally, this discovery led to efforts to block these immune signaling pathways to promote T-cell activation and cancer cell death. The monoclonal antibodies targeting PD-1, PD-L1, and CTLA4 resulted from these efforts — blocking immune signaling pathways and promoting an anti-cancer immune response. Monoclonal antibodies targeting PD-1, PD-L1, and CTLA4 have been approved by the United States Food and Drug Administration for the treatment of many cancer types, including cancers of the lung, esophagus, stomach, liver, colon, kidney, bladder, breast, cervix, and skin. However, they have not been as thoroughly evaluated in blood cancers.
An Overview of Myelodysplastic Neoplasms: The Case for Novel Therapies
Myelodysplastic syndrome (MDS), now called myelodysplastic neoplasms by the World Health Organization (but still abbreviated MDS), is a cancer of the precursor cells of the blood. MDS frequently causes problems in patients by affecting blood cell production, often causing low white blood cells, red blood cells (anemia), or platelets (thrombocytopenia).
Physicians frequently treat MDS according to its risk category. The risk of death from MDS or progression to a more aggressiveform of blood cancer — called acute myeloid leukemia — can be estimated in several ways. MDS risk estimates are usually performed using a risk calculator that accounts for a patient’s blood counts and the genetic changes within the MDS cells. Lower-risk MDS is generally treated with observation, growth factors that stimulate the bone marrow to produce more cells, or other non-chemotherapy drugs that promote blood count maturation, such as luspatercept. In contrast, many physicians frequently treat higher-risk MDS with chemotherapy. Hypomethylating agents, such as azacitidine or decitabine, are the chemotherapy drug class most frequently used in treating higher-risk MDS.
There are very few treatment options for patients with MDS whose disease does not respond to hypomethylating agents. While high-dose chemotherapy followed by stem cell transplant is a curative option, advanced age and significant comorbidities preclude this approach for many patients. Treatment options for relapsed or refractory myelodysplastic syndrome — particularly following hypomethylating agent failure — remain an unmet clinical need.
From Preclinical Insights to Clinical Trials
PD-L1 and CTLA4 are increased in MDS cells treated with hypomethylating agents (Figure 1A). Furthermore, hypomethylating agents decrease the methylation of PD-1 gene promoters, which increases the expression of PD-1 in T cells. Since PD-1, PD-L1, and CTLA4 are increased in MDS following hypomethylating agent therapy, we evaluated the safety and efficacy of therapies that block these pathways in MDS. We hypothesized that these therapies may be useful in patients whose disease
Ipilimumab is a monoclonal antibody targeting the CTLA4 protein on T cells, and nivolumab is a monoclonal antibody that targets the PD-1 receptor on T cells (Figure 1B). We treated 55 patients with MDS whose disease progressed on hypomethylating agents with one of three treatment regimens: ipilimumab, nivolumab, or ipilimumab plus nivolumab. In addition to determining the safety and efficacy of these therapies, we also wanted to test the concept of hypomethylating agent resensitization. Therefore, patients whose MDS did not respond to immunotherapy were retreated with azacitidine while they continued immunotherapy.

Figure 1A PD-L1 and CTLA4 are upregulated on MDS cells and T cells following hypomethylating agent failure. Figure 1B Ipilimumab disrupts the interaction between B7 and CTLA4, while nivolumab interferes with the binding of PD-1 and PD-L1. Both approaches culminate in T-cell mediated immune attack of MDS cells.
Success in Some MDS Types, Failures in Others
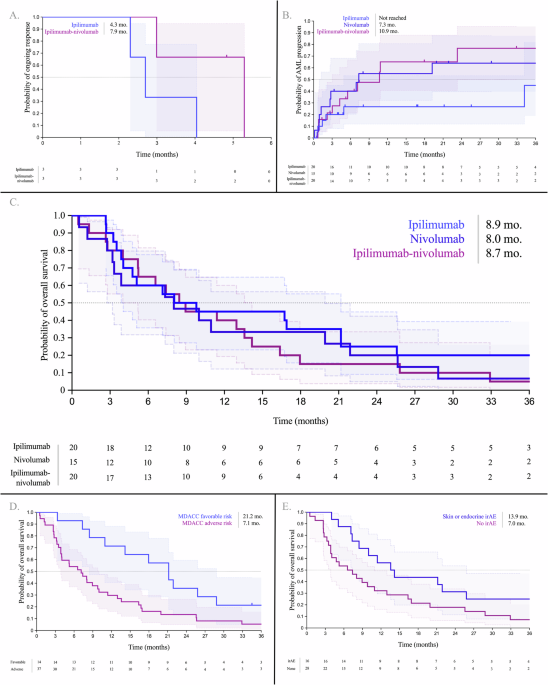
Overall, our study featured a high-risk population of MDS patients. Most were older adults with some degree of medical comorbidities. We observed limited response rates: the overall response rates were 15% for ipilimumab, 0% for nivolumab, and 16% for ipilimumab-nivolumab. However, patients with certain mutations in their MDS cells, such as DNMT3A and ASXL1, were more likely to respond. On the other hand, patients with TET2 mutations were less likely to respond.
A key question of this study was to determine if immunotherapy could resensitize patients to hypomethylating agents. We found that this was not the case. There was no improvement in response rates in patients treated with immunotherapy or azacitidine combined with immunotherapy. However, we observed that patients treated with intensive chemotherapy or venetoclax (a BCL2 small molecule inhibitor) in later lines of therapy had better response rates than with immunotherapy or azacitidine and immunotherapy. These approaches may be more promising avenues for overcoming hypomethylating agent failure.
There was no difference in overall survival among patients treated with any of the three immunotherapy regimens. However, when we combined the cohorts, we observed that patients with TP53, TET2, DNMT3A, loss of chromosome 5, and loss of chromosome 7q had worse overall survival. At the same time, patients with RUNX1 mutations, normal karyotypes, and — surprisingly — complex karyotypes had better overall survival. We used these findings to create a prognostic classification schema for patients treated with immunotherapy called the MD Anderson PD-I model.
Immunotherapy-Related Side Effects in MDS
Since immunotherapy approaches that block the PD-1 and CTLA4 axis activate T cells, a notable event is that these drugs cause side effects from an overactive immune system, also known as immunotherapy-related adverse events (irAEs). However, certain irAEs are associated with better outcomes in solid tumors treated with immunotherapy. Such benefits have not been clearly shown in MDS. In this study, we showed that patients who had skin and endocrine irAEs had improved overall survival. This data is consistent with studies in solid tumors that suggest favorable outcomes in patients with skin irAEs.
Immunotherapy in Hypomethylating Agent Failure MDS: The Takeaway
While the response and survival of patients treated with immunotherapy-based approaches in MDS have been disappointing, our findings define molecular, cytogenetic, and clinical characteristics of patients who may have favorable outcomes.
Follow the Topic
-
Leukemia
This journal publishes high quality, peer reviewed research that covers all aspects of the research and treatment of leukemia and allied diseases. Topics of interest include oncogenes, growth factors, stem cells, leukemia genomics, cell cycle, signal transduction and molecular targets for therapy.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in