JMCR: Clinical Reasoning From Case Reports
Published in Neuroscience and Biomedical Research
Explore the Research
Acute intermittent porphyria presenting as posterior reversible encephalopathy syndrome: a case report
Presentation of Case
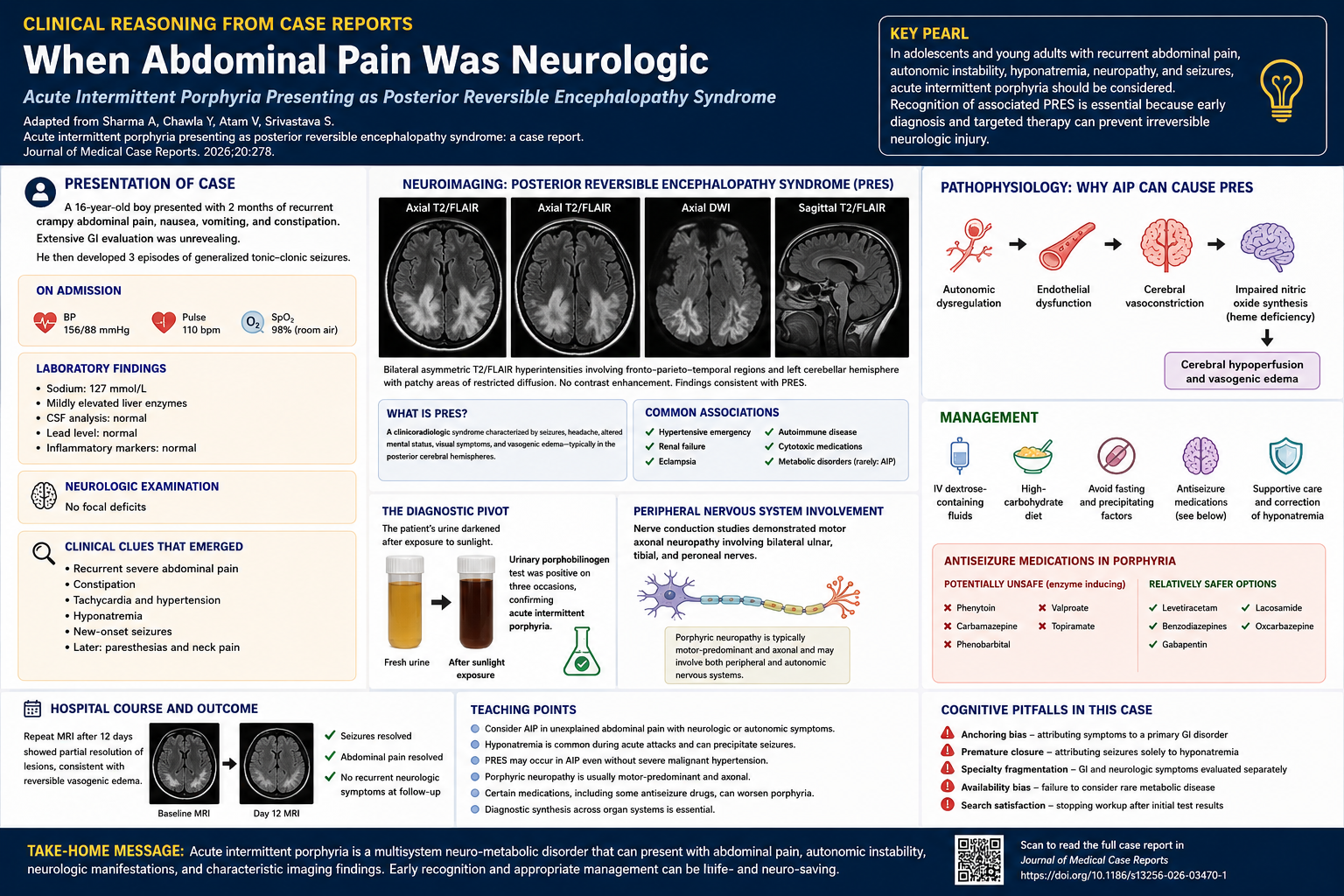
A 16-year-old boy was admitted to the hospital because of recurrent abdominal pain and new-onset seizures.
Two months before admission, intermittent crampy abdominal pain developed. The pain was predominantly periumbilical and was associated with nausea, vomiting, and constipation. The symptoms waxed and waned, occasionally improving spontaneously before recurring. During this period, the patient underwent extensive gastrointestinal evaluation, including abdominal ultrasonography, computed tomography of the abdomen, upper endoscopy, and colonoscopy, all of which were unrevealing.
Forty-eight hours before admission, three episodes of generalized tonic–clonic seizures occurred. Each episode lasted approximately 1 to 2 minutes and was followed by confusion and drowsiness. There was no previous history of seizures, head trauma, psychiatric disease, or neurologic illness. Family history was unremarkable.
On examination, the blood pressure was 156/88 mmHg, the pulse was 110 beats per minute, and the oxygen saturation was 98% while the patient was breathing ambient air. Neurologic examination showed no focal deficits.
Laboratory studies revealed a sodium level of 127 mmol per liter and mildly elevated liver enzyme levels. Cerebrospinal fluid analysis was normal. Testing for lead toxicity was negative.
Magnetic resonance imaging of the brain demonstrated bilateral asymmetric T2/FLAIR hyperintensities involving the fronto-parieto-temporal regions and left cerebellar hemisphere. Patchy areas of restricted diffusion were present. These findings were interpreted as being consistent with posterior reversible encephalopathy syndrome (PRES).
What is the differential diagnosis?
Differential Diagnosis
This adolescent presented with recurrent abdominal pain followed by seizures, autonomic instability, hyponatremia, and characteristic MRI abnormalities. The central challenge in this case is determining whether these findings represent several unrelated processes or one unifying diagnosis.
The prolonged gastrointestinal prodrome initially suggests disorders such as inflammatory bowel disease, peptic disease, pancreatitis, or functional gastrointestinal syndromes. However, the extensive negative evaluation and subsequent development of seizures substantially broaden the differential diagnosis.
The combination of abdominal pain and seizures raises concern for toxic-metabolic disorders. Lead toxicity deserves consideration because it may produce abdominal pain, neuropathy, encephalopathy, and seizures. However, testing for lead exposure was negative.
Autoimmune or inflammatory disorders, including autoimmune encephalitis or vasculitis, may present with seizures and systemic manifestations. However, the absence of inflammatory cerebrospinal fluid findings and normal inflammatory markers make these diagnoses less likely.
The MRI findings suggest PRES, a syndrome rather than a specific disease entity. PRES is most commonly associated with severe hypertension, renal failure, eclampsia, cytotoxic medications, and autoimmune disease. However, none of these explanations fully account for the patient’s prolonged abdominal symptoms and autonomic findings.
At this point, several clues begin to converge:
- recurrent severe abdominal pain,
- constipation,
- tachycardia,
- fluctuating hypertension,
- hyponatremia,
- seizures,
- and later peripheral neuropathic symptoms.
Taken together, these findings strongly suggest an acute hepatic porphyria, particularly acute intermittent porphyria (AIP).
Diagnostic Reasoning
Acute intermittent porphyria is caused by deficiency of hydroxymethylbilane synthase, an enzyme involved in heme biosynthesis. Acute attacks often present with abdominal pain, autonomic instability, psychiatric symptoms, peripheral neuropathy, and seizures.
The neurologic manifestations of AIP are protean and frequently misleading. Patients are commonly evaluated initially by gastroenterologists or psychiatrists before the neurologic syndrome becomes apparent. This delay reflects one of the major cognitive pitfalls in multisystem disease: fragmentation of symptoms across specialties.
In this patient, the elevated blood pressure and tachycardia suggested autonomic nervous system involvement. Hyponatremia further supported a systemic metabolic process and may have contributed to seizure susceptibility.
The MRI findings of PRES are especially notable. PRES has increasingly been recognized as a rare manifestation of acute hepatic porphyrias. The mechanism is incompletely understood but may involve autonomic dysregulation, endothelial dysfunction, cerebral vasoconstriction, and impaired nitric oxide synthesis related to heme deficiency.
A particularly revealing clue emerged when the patient’s urine darkened after exposure to sunlight. The urine images shown on page 3 of the report demonstrate oxidation of porphyrin precursors after light exposure, a classic finding in porphyria.
Three urinary porphobilinogen tests were positive, confirming acute intermittent porphyria.
During hospitalization, the patient developed paresthesias and neck pain. Nerve conduction studies demonstrated motor axonal neuropathy involving multiple peripheral nerves. This finding further supported the diagnosis, since porphyric neuropathy is typically motor-predominant and axonal.
Clinical Diagnosis
Acute intermittent porphyria presenting with posterior reversible encephalopathy syndrome.
Discussion
This case illustrates several important principles in neurologic diagnosis.
First, uncommon diseases often present with common symptoms. Abdominal pain, constipation, anxiety, tachycardia, and seizures are frequently encountered in clinical practice. The challenge lies not in recognizing each symptom individually but in identifying the syndromic pattern that unifies them.
Second, PRES should not be regarded as a final diagnosis. Once PRES is identified radiographically, clinicians must search for the underlying driver. In this case, the imaging abnormalities reflected a broader systemic metabolic disorder.
Third, acute hepatic porphyrias may involve the central nervous system, peripheral nervous system, and autonomic nervous system simultaneously. The coexistence of seizures, dysautonomia, neuropathy, and metabolic abnormalities should prompt consideration of porphyria, particularly when gastrointestinal symptoms are prominent.
This case also highlights an important therapeutic issue. Several antiseizure medications may exacerbate porphyria through hepatic enzyme induction. The patient was treated with lorazepam, levetiracetam, and lacosamide, while potentially porphyrogenic medications were avoided.
Because hematin was unavailable, the patient was managed with high-carbohydrate therapy and dextrose-containing fluids, which suppress hepatic aminolevulinic acid synthase activity and reduce production of toxic porphyrin precursors.
A repeat MRI performed 12 days later demonstrated partial resolution of the lesions, confirming the reversible nature of the process.
At follow-up, the patient remained asymptomatic without recurrent neurologic or abdominal symptoms.
Teaching Points
- Acute intermittent porphyria should be considered in patients with unexplained abdominal pain accompanied by neurologic or autonomic symptoms.
- Hyponatremia is common during acute porphyric attacks and may contribute to seizures.
- PRES may occur in acute hepatic porphyrias even in the absence of severe malignant hypertension.
- Porphyric neuropathy is typically a motor-predominant axonal neuropathy.
- Certain antiseizure medications may worsen porphyria and should be avoided.
- Diagnostic synthesis across organ systems remains one of the neurologist’s most important clinical skills.
Clinical Take-Home Message
In adolescents and young adults with recurrent unexplained abdominal pain, autonomic instability, hyponatremia, neuropathy, and seizures, acute intermittent porphyria should remain high on the differential diagnosis. Recognition of associated posterior reversible encephalopathy syndrome is essential because early diagnosis and targeted metabolic management may prevent irreversible neurologic injury.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports.
Multiple Choice Questions
Question 1
A 16-year-old boy presents with recurrent abdominal pain, constipation, tachycardia, hyponatremia, and generalized tonic–clonic seizures. Which diagnosis best unifies these findings?
A. Autoimmune encephalitis
B. Acute intermittent porphyria
C. Wilson disease
D. Multiple sclerosis
E. Viral encephalitis
Answer
B. Acute intermittent porphyria
Explanation
Acute intermittent porphyria (AIP) classically presents with episodic abdominal pain, autonomic instability (tachycardia and hypertension), neuropsychiatric manifestations, hyponatremia, seizures, and peripheral neuropathy. The multisystem combination of gastrointestinal, autonomic, and neurologic symptoms is highly characteristic.
Question 2
Which MRI finding is most characteristic of posterior reversible encephalopathy syndrome (PRES)?
A. Ring-enhancing temporal lesions
B. Basal ganglia calcifications
C. Posterior-predominant vasogenic edema
D. Diffuse meningeal enhancement
E. Isolated corpus callosum lesions
Answer
C. Posterior-predominant vasogenic edema
Explanation
PRES typically demonstrates bilateral cortical-subcortical T2/FLAIR hyperintensities involving the posterior cerebral hemispheres, reflecting vasogenic edema. In this case, MRI showed bilateral asymmetric hyperintensities involving fronto-parieto-temporal regions and the cerebellum.
Question 3
Which mechanism has been proposed to contribute to PRES in acute intermittent porphyria?
A. Dopamine depletion
B. Autoimmune demyelination
C. Nitric oxide synthase dysfunction
D. Direct viral endothelial invasion
E. Cerebral amyloid angiopathy
Answer
C. Nitric oxide synthase dysfunction
Explanation
One proposed mechanism for PRES in AIP involves heme deficiency impairing nitric oxide synthase activity. Reduced nitric oxide production may lead to cerebral vasoconstriction, hypoperfusion, endothelial dysfunction, and vasogenic edema.
Question 4
Which antiseizure medication is generally considered safer in patients with acute intermittent porphyria?
A. Carbamazepine
B. Phenobarbital
C. Phenytoin
D. Levetiracetam
E. Valproate
Answer
D. Levetiracetam
Explanation
Several antiseizure medications can worsen acute porphyria through hepatic enzyme induction, including phenytoin, carbamazepine, phenobarbital, and valproate. Levetiracetam is considered relatively safer and was successfully used in this case.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in