JMCR: Clinical Reasoning From Case Reports
Published in Neuroscience and Biomedical Research
Presentation of Case
A 78-year-old right-handed woman was referred to the neurology clinic because of progressive difficulty with language.
Approximately one year before her first neurologic evaluation, she began experiencing increasing difficulty retrieving words during conversation. Family members described frequent pauses while speaking and increasing reliance on circumlocutions. Rather than naming objects directly, she would describe their function. Grammar remained intact, speech was fluent, and articulation was normal. There was no evidence of dysarthria, stuttering, or effortful speech production. Everyday comprehension appeared preserved.
Her medical history was notable for long-standing hypertension, type 2 diabetes mellitus, coronary artery disease requiring coronary artery bypass grafting, and hepatic cirrhosis secondary to nonalcoholic steatohepatitis. There was no family history of dementia or neurodegenerative disease.
Initial cognitive testing revealed mild deficits in attention and delayed recall. She was advised to pursue cognitive follow-up but was lost to observation for several years.
When she returned approximately five years later, her symptoms had progressed substantially. Speech had become increasingly hesitant because of word-finding pauses. Family members reported frustration during conversations, increasing social withdrawal, and growing difficulty following complex verbal instructions. Although memory impairment had become more apparent, language dysfunction remained the dominant complaint.
At this stage, what diagnostic possibilities should be considered?
Discussion of Differential Diagnosis
The central diagnostic problem is determining whether language dysfunction represents:
- a manifestation of a generalized dementia syndrome,
- a focal neurodegenerative aphasia,
- a vascular language disorder,
- or a secondary cognitive syndrome related to systemic disease.
The chronology is important.
The earliest symptom was not forgetfulness.
The earliest symptom was difficulty retrieving words.
That observation immediately shifts the discussion away from the most common form of Alzheimer disease and toward disorders affecting dominant hemisphere language networks.
The neurologist's task is to determine precisely which language network is failing.
Is This Typical Alzheimer Disease?
The most common presentation of Alzheimer disease begins with episodic memory impairment arising from dysfunction of medial temporal structures.
Patients forget conversations.
They misplace objects.
They repeat questions.
Language impairment generally emerges later.
This patient followed the opposite trajectory.
Language dysfunction clearly preceded major memory impairment by several years.
Therefore, although Alzheimer disease remains possible, it is unlikely to be presenting in its typical amnestic form.
Is This Vascular Cognitive Impairment?
Several aspects of the history favor vascular disease.
The patient had:
- hypertension,
- diabetes,
- coronary artery disease,
- MRI evidence of small-vessel ischemic disease.
However, vascular cognitive impairment typically produces:
- executive dysfunction,
- slowed processing speed,
- attentional deficits,
- impaired mental flexibility.
It does not usually produce an isolated, slowly progressive aphasic syndrome.
Furthermore, there was no history of stroke, stepwise deterioration, or focal neurological deficits.
Vascular disease may be contributory, but it does not appear to be the primary process.
Is This a Primary Progressive Aphasia?
At this point, primary progressive aphasia (PPA) becomes the leading diagnostic category.
PPA is not a disease but a syndrome characterized by progressive degeneration of language networks.
Three major variants are recognized:
- Nonfluent/Agrammatic Variant
- Semantic Variant
- Logopenic Variant
The remainder of the discussion hinges on determining which subtype best fits the patient's phenotype.
Language Localization
The patient's speech was characterized by:
- frequent pauses,
- word-finding difficulty,
- severe anomia,
- phonemic paraphasias,
- impaired repetition of complex sentences,
- preserved grammar,
- preserved articulation.
These findings provide powerful localization clues.
The deficit is not motor.
The patient knows what she wishes to communicate.
Speech production mechanisms remain intact.
The problem instead involves access to lexical representations and manipulation of phonological information.
These functions localize principally to:
- the left posterior superior temporal gyrus,
- the left inferior parietal lobule,
- the temporoparietal junction,
- phonological working memory networks.
This localization strongly suggests logopenic variant primary progressive aphasia.
Why Not Nonfluent/Agrammatic PPA?
Patients with nonfluent PPA typically demonstrate:
- effortful speech,
- apraxia of speech,
- grammatical simplification,
- agrammatism.
None of these features were present.
Indeed, one of the striking aspects of this case is the preservation of grammatical structure even late in the disease course.
Therefore, nonfluent PPA becomes unlikely.
Why Not Semantic Variant PPA?
Patients with semantic dementia lose conceptual knowledge.
They may no longer understand the meaning of common words.
Object recognition becomes impaired.
Single-word comprehension deteriorates.
In contrast, this patient retained single-word comprehension and object knowledge despite profound naming difficulty.
This distinction is crucial.
Failure to retrieve a word is fundamentally different from failure to understand its meaning.
Thus semantic variant PPA is also unlikely.
The Critical Diagnostic Clue: Sentence Repetition
Among all findings in this case, impaired sentence repetition is perhaps the most diagnostically important.
Many clinicians focus on naming deficits.
However, naming impairment occurs across numerous neurodegenerative disorders.
Sentence repetition is more discriminating.
The patient had disproportionate difficulty repeating long and syntactically complex sentences while preserving motor speech and grammar.
This finding implicates dysfunction of phonological working memory.
Neuroanatomically, these networks reside within the left temporoparietal cortex.
This is the hallmark deficit of logopenic variant PPA.
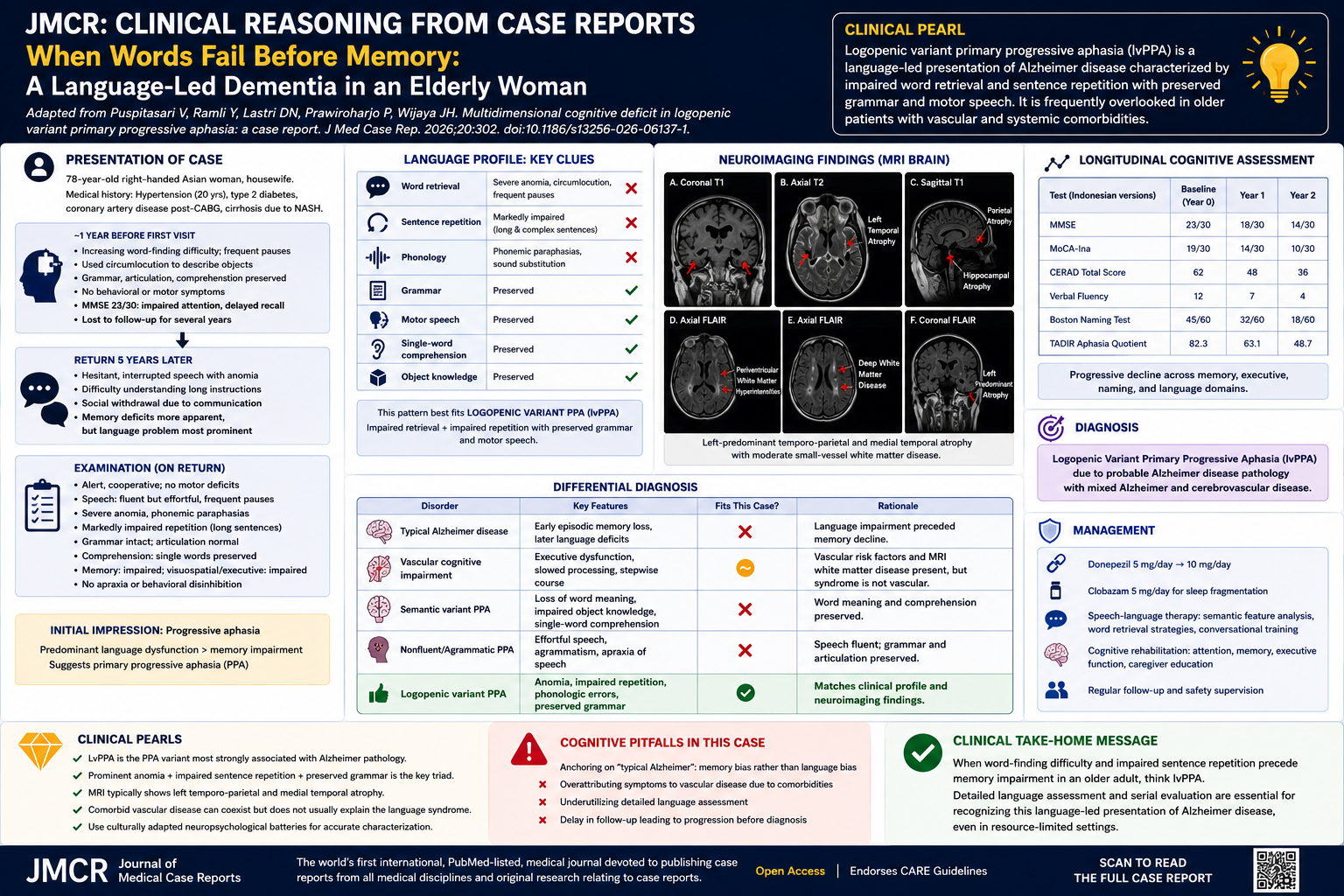
Neuroimaging Correlation
At this point, one would predict MRI abnormalities involving the dominant temporoparietal cortex.
The MRI findings are remarkably congruent with that prediction.
As shown in Figure 1 on page 4, MRI demonstrated:
- left-predominant temporal atrophy,
- left parietal atrophy,
- medial temporal atrophy,
- moderate white matter disease.
The imaging abnormalities localize precisely to the language networks implicated by the bedside examination.
This concordance between examination and imaging substantially strengthens the diagnosis.
One of the most satisfying moments in behavioral neurology occurs when the MRI confirms a localization that was already apparent clinically.
What Is the Underlying Pathology?
Historically, primary progressive aphasia was considered part of the frontotemporal degeneration spectrum.
However, logopenic variant PPA is different.
Among the PPA syndromes, lvPPA is the variant most strongly associated with Alzheimer pathology.
The combination of:
- medial temporal atrophy,
- progressive memory decline,
- temporoparietal degeneration,
further supports underlying Alzheimer disease.
Thus this patient most likely represents:
Alzheimer disease presenting through a language network rather than a memory network.
Final Clinical Diagnosis
Logopenic Variant Primary Progressive Aphasia (lvPPA) due to probable Alzheimer disease pathology occurring in the setting of mixed Alzheimer and cerebrovascular disease.
Clinicopathologic Lessons
This case illustrates several enduring principles of neurologic diagnosis.
First, symptoms should be localized before they are labeled.
Second, language disorders require detailed characterization rather than simple recognition that "speech is impaired."
Third, Alzheimer disease is not synonymous with memory loss.
Different cortical networks may be selectively vulnerable, producing markedly different clinical phenotypes.
Finally, bedside examination remains the foundation of behavioral neurology.
Before any MRI was reviewed, the language profile had already localized the lesion and predicted the diagnosis.
That remains the essence of the CPC tradition.
Clinical Take-Home Message
Progressive word-finding difficulty, impaired sentence repetition, preserved grammar, preserved motor speech, and left temporoparietal atrophy define the logopenic variant of primary progressive aphasia. Although often overlooked as atypical dementia, lvPPA frequently represents a language-led presentation of Alzheimer disease and demonstrates the enduring value of careful bedside language localization in clinical neurology.
Teaching Pearl
The single highest-yield bedside clue to logopenic variant primary progressive aphasia is impaired repetition of long sentences in a patient with preserved grammar and preserved motor speech. When this finding is accompanied by progressive word-finding pauses and left temporoparietal atrophy, clinicians should strongly suspect a language-led presentation of Alzheimer disease.
Question 1
A 78-year-old woman presents with progressive word-finding difficulty, severe anomia, impaired repetition of long sentences, preserved grammar, and preserved motor speech. Which primary progressive aphasia (PPA) subtype is most consistent with this presentation?
A. Nonfluent/Agrammatic Variant PPA
B. Semantic Variant PPA
C. Logopenic Variant PPA
D. Mixed Transcortical Aphasia
E. Global Aphasia
Answer
C. Logopenic Variant PPA
Explanation
Logopenic variant primary progressive aphasia (lvPPA) is characterized by:
- impaired word retrieval,
- impaired sentence repetition,
- phonological errors,
- preserved grammar,
- preserved motor speech.
The patient's prominent anomia, circumlocutions, impaired repetition, and preserved syntax closely fulfill the 2011 Gorno-Tempini diagnostic criteria for lvPPA.
Question 2
Which language feature most strongly distinguishes logopenic variant primary progressive aphasia from semantic variant primary progressive aphasia?
A. Presence of anomia
B. Presence of phonemic paraphasias
C. Impaired sentence repetition with preserved single-word comprehension
D. Progressive cognitive decline
E. Age at onset
Answer
C. Impaired sentence repetition with preserved single-word comprehension
Explanation
Both lvPPA and semantic variant PPA may exhibit naming impairment. However, patients with semantic variant PPA lose semantic knowledge and demonstrate impaired single-word comprehension. In contrast, patients with lvPPA retain word meaning but struggle with sentence repetition because of impaired phonologic working memory. The patient demonstrated preserved word-level comprehension despite severe naming deficits.
Question 3
Which neuroanatomic region is most closely associated with the language deficits observed in logopenic variant primary progressive aphasia?
A. Right frontal operculum
B. Bilateral occipital lobes
C. Left temporoparietal junction
D. Bilateral basal ganglia
E. Cerebellar hemispheres
Answer
C. Left temporoparietal junction
Explanation
Logopenic variant PPA primarily affects the dominant hemisphere language network involving:
- the left posterior temporal cortex,
- inferior parietal lobule,
- temporoparietal junction,
- phonologic working memory circuits.
MRI in this patient demonstrated left-predominant temporal and parietal atrophy, consistent with this localization. The MRI images on page 4 show left temporal and parietal volume loss with associated medial temporal atrophy.
Question 4
Which underlying neuropathologic process is most commonly associated with logopenic variant primary progressive aphasia?
A. Lewy body disease
B. Prion disease
C. Corticobasal degeneration
D. Alzheimer disease pathology
E. Progressive supranuclear palsy
Answer
D. Alzheimer disease pathology
Explanation
Unlike the nonfluent and semantic variants of PPA, which are more frequently associated with frontotemporal lobar degeneration, lvPPA is strongly associated with Alzheimer disease pathology. The patient's medial temporal atrophy, progressive memory impairment, and temporoparietal degeneration support an underlying Alzheimer-type neurodegenerative process.
Question 5
A clinician evaluating this patient prematurely concludes that her cognitive decline is entirely attributable to vascular cognitive impairment because of hypertension, diabetes, and MRI white matter disease. Which cognitive error is being demonstrated?
A. Confirmation bias
B. Anchoring bias
C. Outcome bias
D. Availability bias
E. Hindsight bias
Answer
B. Anchoring bias
Explanation
Anchoring bias occurs when a clinician fixates on an early diagnostic impression and inadequately adjusts despite new information. Although the patient had vascular risk factors and moderate white matter disease, the dominant syndrome was progressive aphasia characterized by severe anomia, phonologic errors, and impaired sentence repetition—features that are far more consistent with lvPPA than isolated vascular cognitive impairment.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.



![When PSMA-targeted therapy is not enough: high-risk localized prostate cancer after repeated [177Lu]Lu-PSMA radioligand therapy](/cdn-cgi/image/metadata=copyright,fit=scale-down,format=auto,quality=95,width=256,height=256/https://public-storage.zapnito.com/Ku6h7Yyp4Q0LXqRRMICCHR2v4LcOsmxMrmDPtOYuI1c)

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in
Amazing post! Wonderfully put together and systematically explained.
Are there any speech-therapy options in these cases?
Dear Lukas,
Thank you for your post and comments. Below is what I obtained from Open Evidence regarding your question:
Yes — several speech-language therapy (SLT) approaches have demonstrated benefit in logopenic variant PPA (lvPPA), though gains are typically partial and most effective when initiated early. The case described already employed two evidence-based strategies (semantic feature analysis and spaced retrieval training), which align well with current literature. Below is a summary of the available options.
Impairment-Based (Restorative) Interventions
Lexical retrieval / naming treatment: A study of 18 individuals with PPA (9 lvPPA) showed significantly improved naming of trained items immediately post-treatment, with maintenance of gains up to 1 year and generalization to untrained items up to 6 months. Notably, once-weekly clinician-directed sessions combined with daily home practice were sufficient — more frequent sessions did not confer additional benefit. This approach leverages spared cognitive-linguistic domains and develops self-cueing strategies. [1]
Semantic feature analysis (SFA): A systematic review of 21 studies (55 participants with aphasia) found that naming of trained items improved in ~82% of participants, with a small overall treatment effect. SFA can also be combined with transcranial direct current stimulation (tDCS) over the left temporoparietal cortex, which showed advantages for trained items and a shallower rate of decline over 6 months compared with untrained items. [2-3]
Phonological short-term memory training: A teletherapy-based study specifically in lvPPA demonstrated significant improvements in immediate and delayed repetition of trained items, though generalization to functional language tasks (picture description, naming) was limited, suggesting the intervention may remain task-specific. This approach directly targets the core phonological loop deficit in lvPPA. [4]
Compensatory and Communication-Based Strategies
Augmentative and alternative communication (AAC): As naming deteriorates, compensatory strategies become essential. Options range from low-tech (pictographic communication boards, written prompts, laminated reference cards) to high-tech (personalized smartphone applications with prerecorded messages). Early introduction of AAC alongside restorative therapy is recommended so that patients and caregivers become familiar with these tools before they are critically needed. [5-6]
Communication partner training: Educating caregivers and family members on how to facilitate communication — using simplified language, allowing extra response time, providing contextual cues, and reducing communication pressure — is a key component of comprehensive PPA management. [5][7]
Script training: Particularly useful for maintaining functional communication in everyday scenarios (e.g., ordering food, greeting visitors), script training involves rehearsing personally relevant conversational scripts. [5][8]
Non-Invasive Brain Stimulation as an Adjunct
A 2024 Cochrane review and a 2025 systematic review noted that tDCS combined with language therapy may improve repetition abilities and cognitive function, while repetitive TMS (rTMS) has shown benefits for naming and speech fluency. [7-8] However, the evidence base remains limited by small sample sizes and heterogeneous study designs, and these modalities are not widely available, particularly in resource-limited settings.
Key Practical Considerations
Impairment-based approaches are most effective when initiated early in the disease course, before severe functional decline. [5] As the disease progresses, the therapeutic emphasis should shift toward compensatory strategies and caregiver support. In the case described, the patient is now at a moderate-to-severe stage (MMSE 9/30), where maximizing functional communication through AAC, environmental modifications, and caregiver-mediated cueing is likely to yield the greatest practical benefit.
1. Treatment for Word Retrieval in Semantic and Logopenic Variants of Primary Progressive Aphasia: Immediate and Long-Term Outcomes. Journal of Speech, Language, and Hearing Research : JSLHR. 2019. Henry ML, Hubbard HI, Grasso SM, et al. 2. A Systematic Review of Semantic Feature Analysis Therapy Studies for Aphasia. Journal of Speech, Language, and Hearing Research : JSLHR. 2018. Efstratiadou EA, Papathanasiou I, Holland R, Archonti A, Hilari K.SR 3. Semantic Feature Training in Combination With Transcranial Direct Current Stimulation (tDCS) for Progressive Anomia. Frontiers in Human Neuroscience. 2016. Hung J, Bauer A, Grossman M, et al. 4. Effectiveness of a Teletherapy-Based Phonological Short-Term Memory Training in Reducing Phonological Impairments in the Logopenic Variant of Primary Progressive Aphasia: A Multiple Case Study. Frontiers in Human Neuroscience. 2025. Duboisdindien G, Lavoie M, Laforce R, Macoir J.Recent 5. Role of the Speech-Language Therapist/Pathologist in Primary Progressive Aphasia. Neurology. Clinical Practice. 2023. Gallée J, Volkmer A. 6. Supporting Communication for Patients With Neurodegenerative Disease. NeuroRehabilitation. 2015. Fried-Oken M, Mooney A, Peters B.Review 7. Non-Pharmacological Interventions for Improving Language and Communication in People With Primary Progressive Aphasia. The Cochrane Database of Systematic Reviews. 2024. Roheger M, Riemann S, Brauer A, et al.SR 8. Safety and Efficacy of Different Therapeutic Interventions for Primary Progressive Aphasia: A Systematic Review. Journal of Clinical Medicine. 2025. Alrasheed AS, Alshamrani RA, Al Ameer AA, et al.Review