Systems analysis identifies endothelin 1 axis blockade for enhancing the anti-tumor effect of multikinase inhibitor
Published in Cancer
Hepatocellular carcinoma (HCC) is the fourth leading cause of cancer-related death in the world. However, effective therapies are limited and improvements are urgently needed. Sorafenib (Nexavar®), a multikinase inhibitor that blocks Raf serine/threonine kinase and receptors for vascular endothelial growth factor (VEGF) and plate derived growth factor (PDGF) tyrosine kinase, is the first-line drug for advanced HCC. However, sorafenib had only modest efficacy, raising a pressing need for prognostic factors that can identify advanced HCC patients that will respond to sorafenib. Although VEGFA, VEGFR, and hypoxia inducible factor 1α (HIF-1α) have been proposed as candidates for the prognostic biomarker of sorafenib responsiveness, there is no clinically useful and easily measurable molecule that can predict the responsiveness and the prognosis of HCC patients under sorafenib treatment.
Endothelins (EDNs) are a family of 21-amino-acid peptides. There are three isoforms: EDN1, EDN2, and EDN3. EDNs are autocrine and paracrine signals that activate the G protein-coupled receptors (GPCRs) endothelin receptor A (EDNRA) and endothelin receptor B (EDNRB). EDN1 and EDN2 bind to EDNRA with various affinities, whereas all three EDN isoforms bind with similar affinity to EDNRB. EDN1 is the most abundant isoform and functions as a vasoactive molecule. In cancers, EDN1 signaling has multiple roles, including the promotion of angiogenesis and of cancer cell proliferation, migration, and invasion, and the inhibition of cell death. Activation of the EDN1-EDNRA axis triggers HCC migration and invasion in human HCC cells. However, the downstream molecular mechanisms by which EDNs and their receptors promote survival, growth, or metastasis of HCC and other cancers remain unknown.
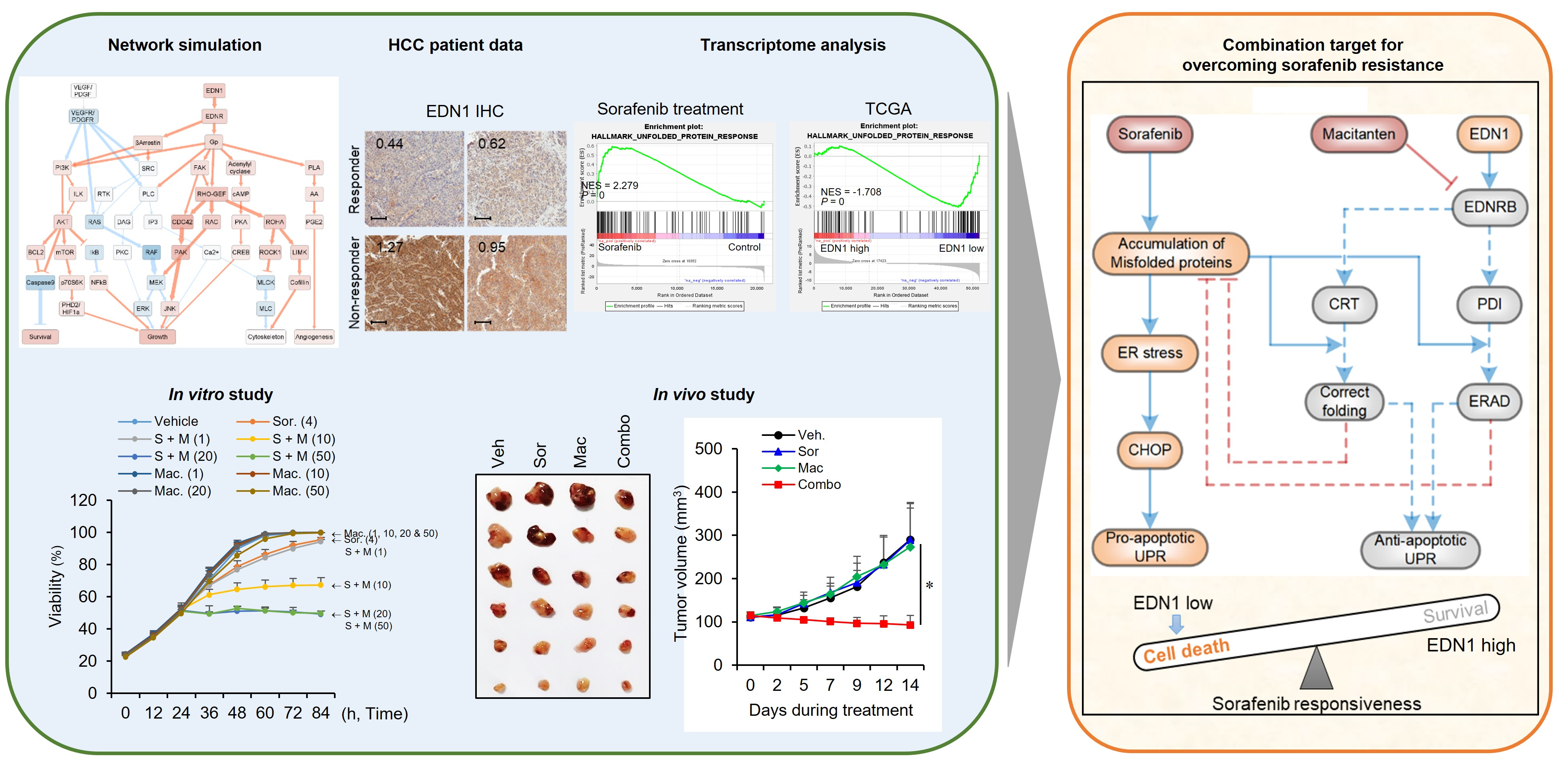
Here, we identified EDN1 has a key indicator of responsiveness to sorafenib treatment in HCC patients. We investigated the oncogenic mechanisms regulated by EDN1 in cancer by comparing gene expression and protein abundance profiles of HCC cell lines and patient tumor samples with high and low amounts of EDN1. Our previous study showed that sorafenib exerts its effect by increasing unfolded protein response (UPR). In this study, it was revealed that EDN1 expression decreased UPR and promoted the poor responsiveness. We found that blocking EDNRB, with either a specific antagonist or a dual EDNR antagonist, restored proteotoxic stress by sorafenib and overcame poor responsiveness to sorafenib.
We constructed a molecular regulatory network model of EDN1 signaling in HCC. With this model, we determined that EDN1 signaling and sorafenib treatment shifted the outcome of the UPR pathway in different directions with EDN1 promoting an anti-apoptotic outcome and sorafenib promoting an apoptotic outcome. However, the combination treatment with dual EDNR antagonist and sorafenib shifted the outcome to a pro-apoptotic response even when EDN1 was overexpressed. In vitro and in vivo experiments confirmed that inhibition of EDN1-EDNRB pathway not only impaired HCC growth but also improved the response to sorafenib, suggesting a promising novel therapeutic strategy for the treatment of advanced HCC. Thus, we identified a prognostic biomarker for stratifying HCC patients for sorafenib treatment and provided preclinical support for the repurposing of macitentan, a dual antagonist of both EDNRA/B currently used for pulmonary artery hypertension, for combinatorial treatment with sorafenib in HCC.
We suggested that EDN1 may be a marker for the prognosis of treatment with sorafenib. Survival analysis revealed that time to progression and overall survival of sorafenib-treated HCC patients are significantly different depending on EDN1 expression. The association with EDN1 expression and prognosis was not observed in HCC patients who were not treated with sorafenib. Thus, EDN1 expression appears to be a specific prognostic indicator of sorafenib response not of HCC progression.
Clinically, measurable serum markers are the most desirable, because tissue samples can be difficult to obtain from HCC patients and intratumoral heterogeneity can confound the analysis. EDN1 is a secreted protein. We found EDN1 is significantly lower in HCC patients that responded to sorafenib than in those that did not, and this was evident both in tissue samples (transcript and protein) and in serum samples obtained prior to the start of treatment. Thus, EDN1 may be a specific serum marker for predicting the response to sorafenib treatment in advanced HCC patients. The diagnostic value of EDN1 still needs further investigation to integrate serum EDN1 levels and various clinicopathologic features. However, our results are encouraging at least with regard to predicting sorafenib responsiveness.
Another translationally important finding is that we identified EDNRB as an effective combination target to enhance the response to sorafenib. We found that the combination of EDNRB antagonists and sorafenib synergistically increased cell death. Our modeling data indicated that sorafenib and EDN1 both regulated the ER stress response and UPR with EDN1 limiting CHOP-mediated apoptosis and thus preventing sorafenib-induced CHOP-dependent cell death. We confirmed that the combination of sorafenib and macitentan, a dual EDNRA/B antagonist, dramatically reduced tumor volume and tumor weight compared to either agent alone and that the combination had no obvious toxicity based on animal weight and serum transaminase measurements.
Our results indicated that the synergistic effects with sorafenib depended on blockade of the EDN1-EDNRB axis, not the EDN1-EDNRA axis. This is consistent with the disappointing outcomes of Phase III clinical trials of EDNRA antagonist (ZD4054) (ENTHUSE M1C; ClinicalTrials.gov NCT00617669). The results of ZD4054 alone or in combination with docetaxel were similar to those of placebo or docetaxel alone in time to progression and overall survival of prostate cancer. However, our study provides support for the repurposing of macitentan, a dual EDNRA and EDNRB antagonist that is currently used for pulmonary artery hypertension, as a combination therapy with sorafenib in advanced HCC patients.
Although we only tested the effect of the combination of sorafenib and EDNRB antagonists on HCC cells, it is possible that these two drugs may also target tumor-associated stromal components, such as fibroblasts, and vascular endothelial, inflammatory, and lymphatic cells. In cancers that are overexpressing EDN1, each of these other cell of the tumor microenviroment also has the potential to respond to EDN1. Our findings will spark additional studies in other types of cancer to assess whether EDN1 is a prognostic indicator of multi-kinase inhibitor responsiveness and whether EDNRB antagonists also enhance the efficacy of sorafenib or other multi-kinase inhibitors in multiple types of tumors.
Follow the Topic
-
Cancer Gene Therapy
The essential gene and cellular therapy resource for cancer researchers and clinicians, keeping readers up to date with the latest developments in gene and cellular therapies for cancer.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in