Uncovering Depression in Lesotho: What a National Survey Revealed About Who Suffers and Who Gets Help
Published in Biomedical Research, General & Internal Medicine, and Public Health

When we started working on this paper, our goal was simple but ambitious: to understand how common major depressive disorder (MDD) symptoms are in Lesotho, what puts people at higher risk, and whether those who are struggling are actually getting any help.
Why we focused on Lesotho
Lesotho is a small, mountainous country in southern Africa, but it carries a disproportionately heavy mental health burden. Previous research had already suggested that depression is common there, and that Lesotho has one of the highest incidence rates of depression globally, yet most existing studies were either clinic-based, focused on very specific groups, or limited to particular regions. At the same time, the country’s mental health system is still developing, with very limited specialized services, few trained professionals, and large gaps in awareness and access.
In 2023–24, something important happened: the Lesotho Demographic and Health Survey (LDHS) included a full mental health module for the first time, including the PHQ‑9 depression screening tool. For us as statisticians and public health researchers, this was an opportunity we could not ignore. It meant we could finally provide a nationally representative picture of depressive symptoms and help‑seeking behavior, not just snapshots from a single clinic or district.
What we set out to do
We designed the study around three main questions:
-
How many people in Lesotho are experiencing symptoms consistent with major depressive disorder?
-
Which groups are more likely to experience these symptoms?
-
Among those with symptoms, who actually seek help or receive medication?
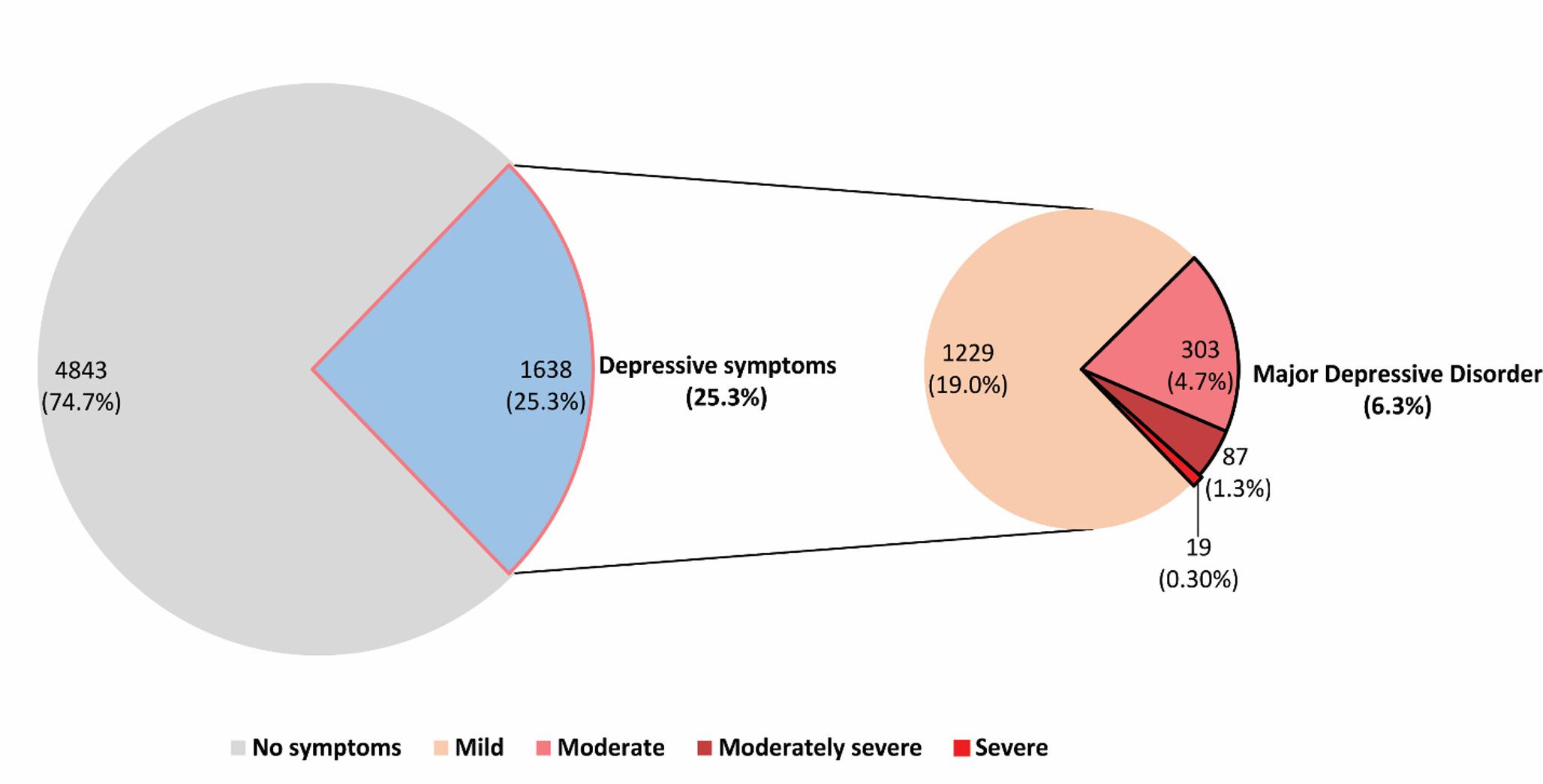
To answer these, we used LDHS 2023–24 data from 6,481 men and women of reproductive age who completed the mental health module. Depression symptoms were measured using the PHQ‑9, and we followed the widely used threshold of a score of 10 or above to define the presence of MDD symptoms. We then applied multilevel mixed‑effects logistic regression to account for the fact that people are nested within households and communities, which can influence their mental health in shared ways.
What we found about depression in Lesotho
One of the most striking findings is that 6.3% of people in our sample had moderate to severe depressive symptoms, high enough to meet the PHQ‑9 threshold for MDD. If you include any depressive symptoms at all, about one in four people showed at least mild symptoms, but most were mild and did not meet the threshold for MDD.
We also found that people living in households with fewer than four members and those who used tobacco had significantly higher odds of MDD symptoms. Smaller households may mean less emotional and social support, fewer people to share financial or caregiving responsibilities, and greater isolation, factors that can erode mental health over time. Tobacco use likely reflects a mix of coping behavior and underlying psychological distress; smoking might feel like a short‑term relief while worsening mood in the longer term.
Another unexpected pattern was geographic. People living in Mohale’s Hoek district had more than three times the odds of experiencing MDD symptoms compared with those in the capital, Maseru, while those in Mokhotlong had substantially lower odds. These differences highlight how local context, poverty, service availability, stigma, and community support can shape mental health in very specific ways, even within one country. Interestingly, rural residence overall was associated with lower odds of MDD symptoms compared with urban areas, which runs against the common assumption that rural areas are always worse off.
The silent crisis: low help‑seeking and treatment
Perhaps the most worrying finding is not just who has MDD symptoms, but what happens next. Among people with any depressive symptoms, only 22.5% had ever tried to seek help, and just 6.5% reported using medication for depression. In other words, roughly four out of five people who are struggling never reach out for assistance, and an even smaller fraction receive pharmacological treatment. Help‑seeking was only slightly higher among women than men, and medication use remained low in both groups. Younger people, especially adolescents aged 15–19, were the least likely to seek help or use medication, while mid‑older adults (45–49 years) had the highest rates of care‑seeking. This suggests that young people in Lesotho may be facing stigma, lack of knowledge, or limited autonomy in decision‑making about their own health, all of which suppress their access to care.
Socioeconomic gradients were also evident. Those in the richest wealth quintile were more likely to seek help and to use medication than those in the poorest quintile. Urban residents were more likely than rural residents to access services, reflecting a higher concentration of facilities and providers in cities. And districts differed markedly: help‑seeking and medication use were higher in places like Butha‑Buthe and Leribe, and much lower in Mokhotlong. These patterns show that the mental health treatment gap is not just about individual behavior; it is deeply tied to geography, poverty, and the structure of the health system.
How we approached the analysis
From a methodological point of view, this study was a chance to bring rigorous statistical tools to a real‑world mental health problem in a low‑resource setting. We used DHS survey weights and design variables to ensure that our estimates represented the national population, accounting for the complex, multi‑stage sampling design of LDHS. We then applied multilevel mixed‑effects logistic regression, which allowed us to capture differences not only between individuals but also between communities and districts.
We followed a stepwise modeling strategy: starting from an empty model, then adding individual‑level variables, then household and contextual variables, and finally all covariates together. This framework helped us quantify how much of the variation in MDD symptoms lies at the community level, and how much can be explained by individual and household characteristics. The PHQ‑9 showed high internal consistency in this dataset (Cronbach’s alpha 0.85), which provided confidence in using it as a screening tool in this setting. At the same time, we remained cautious about what the data can and cannot tell us. This is a cross‑sectional survey, so we cannot prove causality, only associations. And because the data are self‑reported, stigma, misunderstanding, and recall issues may influence how people respond.
What this means for mental health in Lesotho
Taken together, our findings point to a clear message: depression is a substantial and unevenly distributed burden in Lesotho, and the vast majority of those affected are not receiving care. Women, tobacco users, people in smaller households, and residents of districts like Mohale’s Hoek are at particularly high risk, yet help‑seeking remains low across almost all groups.
For policymakers and program planners, this suggests several priorities:
-
Strengthen community‑based and primary care mental health services so that people can get help close to where they live.
-
Target high‑risk groups, especially women, tobacco users, and residents of high‑burden districts, with tailored, culturally sensitive interventions.
-
Invest in public awareness campaigns to reduce stigma and improve mental health literacy, particularly among young people.
-
Address geographic inequities by improving access and affordability of services and medications in underserved districts.
-
Build monitoring and evaluation systems into mental health programs to track progress and refine strategies over time.
From a broader perspective, this paper is part of a growing body of work arguing that mental health must be treated as a core public health priority, not an afterthought. For Lesotho, integrating mental health into primary care and community health platforms, while leveraging the new LDHS mental health data, offers a realistic path to narrowing the treatment gap and supporting those quietly living with depression.
If you are interested in the full set of results, including detailed tables, district‑level patterns, and model outputs, you can find them in our article, “Prevalence, determinants, and help‑seeking behavior for major depressive disorder symptoms in the Lesotho population: A multilevel analysis from the Lesotho Demographic and Health Survey 2023–24,” published in Social Psychiatry and Psychiatric Epidemiology
Follow the Topic
-
Social Psychiatry and Psychiatric Epidemiology

This is a scholarly journal dedicated to diverse aspects of psychiatric disorders' epidemiology and particularly social, biological, and genetic dimensions.
Related Collections
With Collections, you can get published faster and increase your visibility.
Social Theory Corner
The social dimension of mental health is conceptualized and acted on by diverse knowledge communities ranging from academic disciplines and health and welfare services to community organizations, patient advocacy, and user-led groups. Those working in these spaces share an interest in how structural, economic, ecological, moral, and political factors impinge upon mental wellbeing, even as differences between them have also catalyzed vital new concepts and methods. Concern with the social determinants of mental health draws attention to key concepts such as intersectionality, social stratification, social capital and social justice and, in turn, paves the way for participatory methods, co-production, data sovereignty, ecosocial theory, and decoloniality in mental health research.
The Social Theory Corner seeks to foster a sustainable space for these collaborative and interdisciplinary exchanges, and for the inclusion of voices and topics traditionally left out of psychiatric research, clinical work, and social theory development. It builds on the recent Special Issue “Theorizing the “social” in mental health research and action” in Social Psychiatry and Psychiatric Epidemiology (SPPE), which was based on a two-year interdisciplinary workshopping process. The Corner creates a permanent home for these conversations, inviting research articles, commentaries and creative contributions that demonstrate reflexivity, critical thinking, and epistemic diversity, and the central importance of social theory in identifying research questions, guiding study designs, and aiding the interpretation of quantitative and qualitative data.
The Corner is particularly interested in contributions that reflect on how key concepts in mental health research can inform change, broadly conceived. We invite authors to widen the discussion of what needs changing to improve mental wellbeing: not only mental health outcomes or their immediate social risk factors but also complex social worlds, political processes, and knowledge infrastructures. By opening up a space for theoretical debate and critical thinking in our journal, we aim to make epidemiology and social theory-development more inclusive and accountable – to real world change, and most importantly, to the people experiencing mental health problems and their communities.
Publishing Model: Hybrid
Deadline: Ongoing
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in