Unequal air, unequal risks: uncovering Europe’s hidden disparities in pollution-related mortality
Published in Earth & Environment and Public Health

This simple question marked the starting point of our study.
By analyzing daily mortality data covering 88.8 million deaths across 653 regions in 31 European countries between 2003 and 2019, we uncovered unknown spatial disparities in vulnerability to air pollution. This continental-scale dataset, developed within the EARLY-ADAPT project, encompasses both urban and rural populations — representing 521 million people over 17 years — allowing us to move beyond city-based analyses and investigate how vulnerability varies across diverse socioeconomic and energy contexts.
What we found reveals a story not only about pollution, but about inequality.
Looking beyond exposure: vulnerability matters
Air pollution does not affect everyone equally. Two regions with similar pollution levels may experience very different health impacts. Why?
The answer lies in vulnerability.
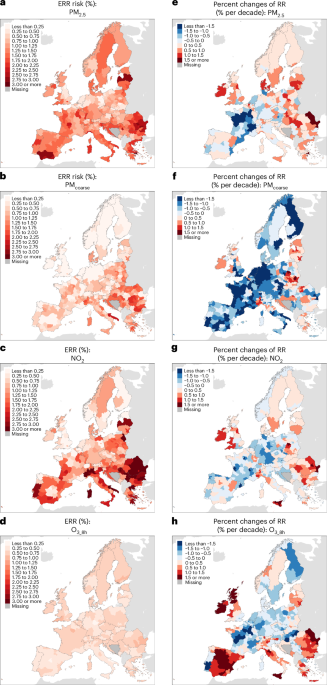
We estimated short-term mortality risks associated with four major pollutants — PM₂.₅, PMcoarse, NO₂, and O₃ — using time-varying epidemiological models, and then examined whether socioeconomic conditions help explain why some regions experience higher mortality risks than others.
The results were striking.Regions with lower GDP per capita, higher poverty rates, lower education levels, and shorter life expectancy — predominantly in Eastern and Southern Europe — faced consistently higher mortality risks. In some cases, the excess relative risks were nearly twice as high as in wealthier regions.
Crucially, disparities were not limited to baseline levels. Over time, more advantaged regions tended to experience declining pollution-related risks, whereas disadvantaged regions often showed weaker improvements — and in some instances, increasing risks. We describe this as a “double burden”: higher vulnerability and weaker capacity for improvement.
Importantly, these disparities persisted when regions were exposed to similar pollution levels. They likely reflect broader structural conditions, including healthcare capacity, environmental governance, demographic change, and co-existing exposures.
The role of the energy transition
We then asked a second question: does the renewable energy transition influence these patterns?
To answer this, we examined renewable energy in two complementary ways — as an upstream driver of pollution exposure and as a potential modifier of vulnerability.
Through counterfactual analyses, we compared observed renewable adoption with a scenario in which countries had remained at their 2004 renewable shares. Without the observed growth in renewable energy, pollutant concentrations in 2019 would have been substantially higher. Correspondingly, attributable mortality would have been 12–53% higher, depending on the pollutant.This suggests that the renewable transition has already contributed to measurable public health gains by reducing exposure.
But the story did not stop there.Regions with higher renewable energy shares — especially those that adopted renewables more rapidly — also showed lower short-term mortality risks per unit of pollution exposure. In other words, renewable transition appeared to be associated not only with cleaner air, but also with reduced vulnerability.
This does not imply a direct biological effect of renewable energy itself. Rather, renewable adoption is often embedded within broader policy frameworks: cleaner transport systems, improved urban design, stronger emissions controls, and sustained environmental governance. In this sense, renewable transition may act as a marker of wider structural modernization. While our analyses do not establish causality, the consistency of associations across pollutants and regions suggests that energy transition and vulnerability are closely intertwined.
A geography of uneven progress
The spatial pattern of our findings is difficult to ignore. Northern and Western European regions generally showed higher renewable shares, lower fossil fuel dependence, lower mortality risks, and stronger declines over time. In contrast, several Eastern and Southern regions faced higher poverty, greater fossil reliance, higher attributable mortality burdens, and weaker improvements.These patterns reflect long-standing structural differences — industrial legacies, coal dependence, economic constraints, and uneven investment capacity.
They also raise an important policy question: are climate and air quality policies delivering health benefits equitably across Europe? Our results suggest that progress has been uneven. As Europe advances toward net-zero targets under the Green Deal and related policy packages, it will be critical to consider not only overall emission reductions, but also the distribution of health benefits. Embedding equity into energy and environmental strategies may require targeted investments in high-burden regions, stronger public health infrastructure, and integration of health impact metrics into climate policy evaluation.
Looking forward
Although our study focuses on Europe, similar patterns may exist elsewhere. In many low- and middle-income countries, rapid urbanization and industrial growth outpace investments in clean energy and public health protection.Air pollution is not only an environmental issue— it is also a social one. Even as average air quality improves, vulnerable populations may remain at disproportionate risk and benefit less from progress. Cleaner air alone is not sufficient. What matters is whether policy can translate into equitablehealth gains, especially for those most vulnerable.
Follow the Topic
-
Nature Medicine
This journal encompasses original research ranging from new concepts in human biology and disease pathogenesis to new therapeutic modalities and drug development, to all phases of clinical work, as well as innovative technologies aimed at improving human health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Clinical Research in Respiratory Medicine
Publishing Model: Hybrid
Deadline: Feb 18, 2027
Cancer Prevention and Control
Publishing Model: Hybrid
Deadline: Feb 19, 2027

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in