When a curable cancer becomes an emergency: understanding early death in metastatic germ cell tumours.
Published in Biomedical Research
Case presentation
A young man arrives at the hospital breathless, coughing blood, and frightened. Only a few weeks earlier, he had considered himself healthy. Now, imaging shows innumerable lung metastases, tumour markers are markedly elevated, and the clinical picture is immediately alarming. The diagnosis is metastatic testicular germ cell tumour, a cancer we deem highly curable.
Treatment must start urgently. Waiting may be fatal. However, chemotherapy itself can cause a fatal complication. In patients with extensive lung metastases, the first days after chemotherapy can trigger rapid respiratory deterioration, lung hemorrhage, infection, or the need for mechanical ventilation. This is one of the most difficult situations in germ cell tumour oncology: the cancer is potentially curable, but the patient may not survive long enough to benefit from cure.
This opening case is a composite, anonymized clinical scenario derived from routine clinical practice and reflects the phenotype investigated in our study.
The reality of “super-high-risk” patients
For clinicians treating germ cell tumours, such patients are unforgettable. They challenge the usual narrative of this disease. TGCTs are among the major success stories of modern oncology since the advent of cisplatin-based chemotherapy. Yet a small group deteriorates rapidly, sometimes within days of starting treatment. This time, chemoresistance is sparsely the cause of death, but the combination of advanced tumour burden, organ compromise, infection, bleeding, respiratory failure, and treatment-related stress seems to be the culprit.
These patients are rarely represented in clinical trials. They may deteriorate before the first response assessment, before complete histological documentation, or even before all planned staging investigations are completed. Consequently, their experience is often missing from the evidence base that guides treatment decisions.
This gap was the reason for our international study through the Global Society for Rare GU Tumors. Because early death in TGCTs is rare, no single centre can easily answer these questions. We therefore collected data from multiple expert centres on patients with metastatic germ cell tumours who died early after the start of first-line chemotherapy.
In total, we identified 102 patients. This represented a small proportion of all treated cases — less than 2% - but the clinical impact of these events is enormous. Most patients had non-seminomatous germ cell tumours, and many had poor-risk disease according to standard IGCCCG criteria. Lung metastases, liver metastases, markedly elevated tumour markers and impaired clinical status were common.
What we found: the 30-day danger window
Our international cohort revealed several critical insights.
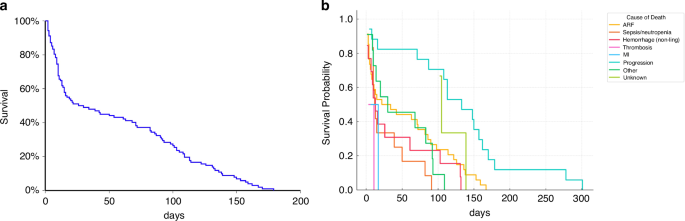
First, the danger window was very short. The median time from the start of platinum-based chemotherapy to death was only 28 days, that means, that approximately half of the patients dying within the first 30 days after starting of chemotherapy. For these patients, the critical period is not months into treatment, but the first days and weeks.
Second, the most frequent cause of early death was acute respiratory failure, followed by disease progression, septic shock with neutropenia, fatal haemorrhage, pulmonary embolism, myocardial infarction and other causes.
Third, acute respiratory failure was more clearly associated with clinical features — extensive lung involvement, resting dyspnoea and haemoptysis - than with choriocarcinoma histology alone. The traditional term “choriocarcinoma syndrome” may therefore not fully capture the broader spectrum of respiratory complications seen in these critically ill patients.
The clinical takeaway is simple: clinicians should not wait for a textbook definition. A patient with a germ cell tumour, massive lung disease, dyspnoea or haemoptysis should be considered super-high risk, regardless of whether choriocarcinoma has already been proven histologically (see Figure).

Figure - Conceptual model of respiratory failure after chemotherapy initiation in metastatic TGCTs with extensive pulmonary involvement. Patients with massive pulmonary involvement have limited respiratory reserve even before treatment initiation. Afterwards, rapid tumor destruction within lung metastases may induce release of inflammatory mediators and tumor-related factors, leading to cytokine production, immune-cell recruitment, alveolar–capillary barrier disruption, and diffuse alveolar damage. This may result in a self- amplifying inflammatory response resembling a cytokine storm, with progression to ARDS and early respiratory death. ARDS, acute respiratory distress syndrome
Another important observation was that very early deaths - those occurring within 30 days - were more often linked to acute complications such as respiratory failure, haemorrhage, infection or cardiovascular events. Later deaths were more often related to disease progression. This distinction matters, because some early complications may be modifiable if anticipated and managed aggressively.
The dilemma of treatment intensity
One of the hardest questions in this setting is how to start chemotherapy safely. Full-dose cisplatin-based chemotherapy offers the best chance of cure, but in patients with massive tumour burden and fragile organ function, it may trigger rapid deterioration. On the other hand, reducing the first dose with the goal of reducing toxicity and complications may result in undertreating a potentially curable cancer.
In our cohort, initial dose reduction was common, particularly in patients with extensive lung involvement or very advanced disease. Patients who received reduced-intensity treatment had worse survival, but this finding must be interpreted cautiously. It almost certainly reflects selection bias: clinicians reduced treatment because these patients were already critically ill. The data do not prove that dose reduction causes worse outcomes. Rather, they highlight how difficult these decisions are and how urgently prospective evidence is needed.
Strategies such as modified induction regimens, delayed bleomycin, initial dose attenuation or stepwise escalation have been explored in selected settings, but robust multicenter prospective validation remains limited. For now, decisions must be individualized and ideally made in experienced centers with access to intensive care, pulmonary support, infectious disease expertise and rapid multidisciplinary assessment.
Moving towards “emergency-style” oncology
Our study reinforces the concept that within the broad category of poor-risk germ cell tumours, there is an even more vulnerable “super-high-risk” group. These are patients in whom the immediate threat is not only long-term relapse or treatment resistance, but early clinical collapse.
Features that should raise concern include massive lung involvement, resting dyspnoea, haemoptysis, liver metastases, very high β-hCG, poor performance status, systemic inflammation, and the need for early ventilatory or ICU support.
For such patients, standard oncological management may not suffice. They may need emergency-style oncology care: immediate triage to high-volume expert centers, early ICU consultation before intubation becomes unavoidable, proactive infection management, careful decisions about induction chemotherapy, G-CSF where appropriate, individualized thromboprophylaxis, and very close monitoring during the first days of treatment.
The key message is simple: cure is still possible, but the window to act may be very short. In these patients, the question is shifting from how to cure the cancer to how to ensure the patient stays alive till the systemic treatment takes effect.
This study is retrospective and has limitations. Some data were incomplete, causes of death were sometimes difficult to classify, and treatment decisions varied between centers. But these limitations also reflect real-world practice. These are precisely the patients who are difficult to study prospectively because they are unstable, urgent and often excluded from trials.
The next step should be to develop practical risk stratification tools and prospective registries focused specifically on early complications. We need harmonized protocols for triage, ICU referral, antimicrobial therapy, respiratory monitoring and adapted induction chemotherapy.
Testicular germ cell tumours remain among the most curable solid cancers. But the success of this field should not make us overlook the patients who die before cure becomes possible. By studying early death, we hope to shift attention to the first critical days of treatment, and ultimately prevent avoidable deaths in a disease where cure is otherwise within reach.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in