Why does direct tumor-adipocyte interaction matter in colorectal cancer pathology?
Published in Cancer
Starting point: accurate patient stratification in colorectal cancer is still a pressing clinical need
With nearly 2 million new cases very year, colorectal cancer (CRC) is the third most common cancer 1, and although five-year overall survival (OS) rate is considerably high for early stages, this rate rapidly decreases for later stages.
Due to its high frequency, we as pathologists diagnose and evaluate CRC specimens basically every day in routine clinical practice. By providing accurate diagnosis and detailed information on the tumor biology (TNM stage, grading, histologic subtype, microsatellite status, mutational status etc.), we pathologists support clinicians in identifying high-risk patients for consecutive (tailored) adjuvant therapy. Unfortunately, disease outcomes in CRC are really heterogenous, even within the same stage group 2. To address the clinical need for a more accurate patient stratification, many different gene-expression based or deep-learning (DL) based approaches have been established recently 3-6. However, despite promising results these methods have not found their way into the clinical routine yet, as they often are time- as well as cost-intensive.
Our solution: SARIFA as new and easy-to-assess, solely H&E-based histopathologic biomarker
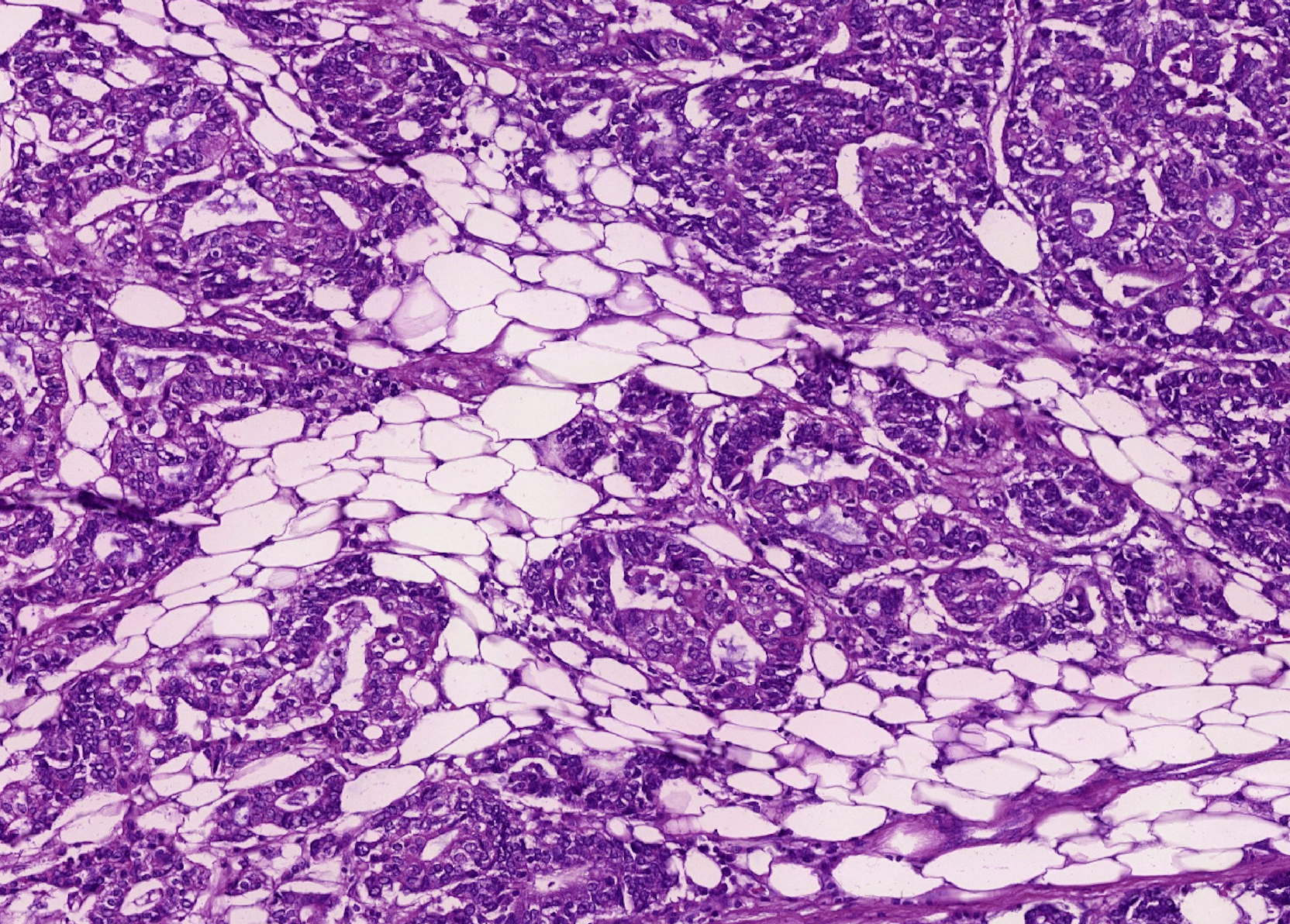
Based on our daily histopathologic experience and the key role of the invasion front in CRC 7, we in Augsburg (Pathology & Molecular Diagnostics, University Hospital Augsburg, led by Prof. Dr. B. Märkl) could establish Stroma AReactive Invasion Front Areas (SARIFA) as novel solely hematoxylin-and-eosin (H&E)-based histopathologic biomarker in colon as well as gastric cancer 8, 9. SARIFA is defined by the direct interaction between tumor cells and adipocytes at the invasion front, without an intervening desmoplastic reaction or inflammatory infiltrate. Assessment of SARIFA-status on for every cancer patient available H&E slides has multiple advantages 8, 9: 1. A very low interobersever variability, 2. No need for further testing (for example via immunohistochemistry or molecular diagnostics) and consecutively almost no additional costs (except pathologist’s time), 3. A really fast assessment (around 20 seconds) and therefore no delay in turnaround time. Moreover, we have provided first evidence that SARIFA-positivity is not only a prognostic feature but also hints at a distinct underlying tumor biology. On the one hand, we could prove a tumor-promoting upregulation of lipid metabolism in SARIFA-positive gastric cancers 9. On the other hand, we observed immunological alterations in SARIFA-positive colorectal cancer patients, especially a substantial decrease in natural killer (NK) cells in the peripheral blood – indicating a reduced anti-tumor immunity 10. The potential link between SARIFA-positivity and immune dysregulation could also be validated by us with regards to gastric cancer 11. Despite all these interesting findings, our novel biomarker SARIFA and has not been comprehensively investigated from a molecular point of view. Furthermore, a widespread adoption of our concept has not taken place yet.
Current study: investigation of SARIFA-status in publicly available TCGA cohorts COAD and READ
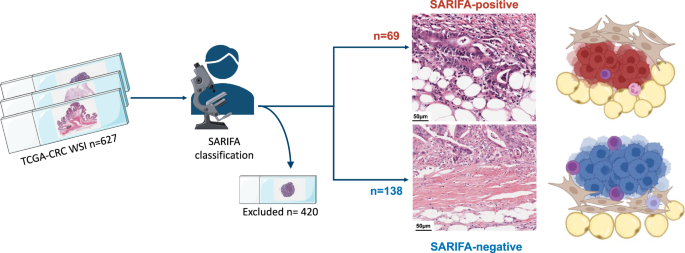
For this publication, we screened the publicly available whole slide images (WSI) of the The-Cancer-Genome-Atlas (TCGA) cohorts COAD (colonic adenocarcinoma) and READ (rectal adenocarcinoma) 12 for the presence or absence of SARIFA (portal.gdc.cancer.gov). After excluding all cases, in which the invasion front is not properly displayed (and for example only superficial tumor parts), we ended up with a cohort of 207 CRC cases with a SARIFA-frequency of 33.3%, which is really close to what have observed in our previous works, indicating that our histopathologic workup of the consistently scalable, high-quality TCGA-WSIs was reliable.
SARIFA-positivity is strongly associated with poor outcomes
Again, SARIFA-positivity was associated with known high-risk features such as higher pT stage, lymph node and distant metastasis. Patients with SARIFA-positive CRCs were characterized by a reduced OS, disease-specific survival (DSS) and progression-free survival (PFS). This strong association between SARIFA-status and outcomes remained true upon multivariate cox regression analysis.
SARIFA-positivity seemingly does not rely on genetic alterations
The extensive molecular data associated with the TCGA enabled us to investigate if SARIFA-status is linked to or even driven by specific high-risk mutations, such as BRAF V600E. Interestingly, SARIFA-positivity seemingly was not associated with any specific mutational profile in this dataset. These findings are completely in line with our previous findings, that were based on a really small cohort (n=45) and targeted panel sequencing covering around 50 genes 10.
SARIFA-positive CRCs show a characteristic gene and protein expression
As we could found no changes on a genomic level, we next asked if SARIFA-positive CRCs are biologically really different from SARIFA-negative CRCs. Therefore, we performed differential gene expression analysis on bulk mRNA data. Here, we could identify a broad dysregulation of gene expression with 731 genes differentially expressed in SARIFA-positive CRCs (with q<0.01, and no LFC threshold), indicating that SARIFA-positivity is indeed associated with a distinct tumor biology. This was also true on a protein level.
What does this tumor biology look like? SARIFA-positive CRCs revealed an enrichment of extracellular matrix and proteoglycan signaling pathways, and were more often of CMS1 (consensus molecular subtype 1, MSI immune) and CMS4 (consensus molecular subtype 4, mesenchymal) and showed higher stromal intensity infiltration scores. Besides this important stromal/mesenchymal component, FABP4 and CD36 were once again upregulated – we know these two key players in lipid metabolism really well as we could also observe an increase of FABP4 and CD36 in gastric cancer on (spatial and bulk) mRNA and protein level 9, 11.
Does this ultimately matter to patients? Potentially yes, as SARIFA may indicate a differential treatment response.
Whereas there is no wrong in identifying prognostic biomarkers, identifying predictive biomarker is what ultimately matters to improve patient outcomes.
Firstly, we firmly believe that our data justifies SARIFA-positivity to be considered as a high-risk feature that could trigger adjuvant chemotherapy in stage II CRCs (of course, this needs to be validated in post-hoc analysis as well as prospective trials). Secondly, differences in gene expression are also likely to result in a differential treatment response, which we could prove by deploying oncoPredict 13 as computational tool for drug response prediction. As SARIFA-positive CRCs are predicted to be more resistant to oxaliplatin and as oxaliplatin is part of most chemotherapy regimens in CRC, our findings could have important clinical consequences. Thirdly, the role of immunotherapy in CRC is increasing year by year. Some data even suggests that not only dMMR/MSI CRCs but also some pMMR/MSS CRCs benefit heavily from immunotherapy 14. However, predictive biomarkers are lacking. With our recently observed changes in immunity in SARIFA-positive cases, immunotherapy could here also be a good option for this particular aggressive subset of CRCs.

Lessons learned and outlook
Our current study could validate SARIFA-status as independent and highly negative prognostic histopathologic biomarker in CRC that is likely the morphologic equivalent of an underlying aggressive tumor biology with its own transcriptional identity. Direct tumor-adipocyte interaction should be considered as a very important morphologic feature, that has mostly been neglected in histopathologic studies in the past.
As we make our SARIFA-classification of the TCGA-CRC cohort with this publication publicly available, this can be used as a training resource as well as starting point for pathologists and researchers globally. More broadly, our studies is a paradigmatic example how publicly available datasets with high-quality histopathologic WSIs can form the basis for comprehensive morphological-molecular association studies with potential clinical consequences.
We firmly believe that SARIFA-status assessment should be implemented into the routine pathologic workup of CRC specimens straightway as it does not produce additional costs but only leads to a gain in information.
References
- Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer. J. Clin. 71, 209-249 (2021).
- Kim, H. S. et al. Clinicopathological and biomolecular characteristics of stage IIB/IIC and stage IIIA colon cancer: Insight into the survival paradox. J. Surg. Oncol. 120, 423-430 (2019).
- Guinney, J. et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 21, 1350-1356 (2015).
- Brunac, A. et al. CINSARC signature outperforms gold-standard TNM staging and consensus molecular subtypes for clinical outcome in stage II-III colorectal carcinoma. Mod. Pathol. 35, 2002-2010 (2022).
- Wulczyn, E. et al. Interpretable survival prediction for colorectal cancer using deep learning. NPJ Digit. Med. 4, 71-2 (2021).
- Foersch, S. et al. Multistain deep learning for prediction of prognosis and therapy response in colorectal cancer. Nat. Med. (2023).
- Koelzer, V. H. & Lugli, A. The tumor border configuration of colorectal cancer as a histomorphological prognostic indicator. Front. Oncol. 4, 29 (2014).
- Martin, B. et al. Stroma AReactive Invasion Front Areas (SARIFA)-A New Easily to Determine Biomarker in Colon Cancer-Results of a Retrospective Study. Cancers (Basel) 13, 10.3390/cancers13194880 (2021).
- Grosser, B. et al. Stroma AReactive Invasion Front Areas (SARIFA) - a new prognostic biomarker in gastric cancer related to tumor-promoting adipocytes. J. Pathol. 256, 71-82 (2022).
- Reitsam, N. G. et al. Alterations in Natural Killer Cells in Colorectal Cancer Patients with Stroma AReactive Invasion Front Areas (SARIFA). Cancers (Basel) 15, 994. doi: 10.3390/cancers15030994 (2023).
- Grosser, B. et al. Stroma AReactive Invasion Front Areas (SARIFA) proves prognostic relevance in gastric carcinoma and is based on a tumor-adipocyte interaction indicating an altered immune response. Gastric Cancer. (2023).
- Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 487, 330-337 (2012).
- Maeser, D., Gruener, R. F. & Huang, R. S. oncoPredict: an R package for predicting in vivo or cancer patient drug response and biomarkers from cell line screening data. Brief Bioinform 22, bbab260. doi: 10.1093/bib/bbab260 (2021).
- Chalabi, M. et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat. Med. 26, 566-576 (2020).
Follow the Topic
-
Cancer Gene Therapy
The essential gene and cellular therapy resource for cancer researchers and clinicians, keeping readers up to date with the latest developments in gene and cellular therapies for cancer.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in