Why quality measures for chiropractic care are important and what we’re doing about it
Published in Healthcare & Nursing and Mechanical Engineering

Scientific evidence supporting chiropractic care has grown substantially over the past several decades. Likewise, care standards now describe key aspects of how care should be delivered. Though much more research will always be needed, current knowledge should not be ignored. Instead, there is a responsibility to pay attention to it, to use it to inform and improve clinical practice.
Quality improvement is a time-honored way to apply current knowledge to improve healthcare. It is achieved by measuring features of health organizations, clinical processes, outcomes, and patient experiences to obtain data about what is working well, what isn’t, and what changes are needed. Quality improvement depends on objective and valid measures called quality indicators/measures.
Why we started
Several years ago, we recognized that no broad set of quality measures for chiropractic care were available. Without these measures, quality improvement may not occur. Failing to act avoids an ethical obligation to objectively evaluate and improve care. Organizations that assessed quality lacked valid measures, which limited interpretation and prevented comparison across settings. Neither option adequately supported objective and sustained improvement over time.
In North America, the Council on Chiropractic Education (CCE) is the main accreditor for Doctor of Chiropractic degree and residency programs. Accredited programs must demonstrate quality improvement in clinical care settings. Standardized, evidence-based, and valid quality measures are ideal for supporting such processes. Several other reasons for developing quality measures include:
- Offering objective data on the effectiveness of care
- Revealing inefficiencies and ineffective policies, infrastructure, and practices
- Providing data to facilitate compliance with regulatory bodies
- Supplying a method to help assess chiropractic integration into a health organization
- Learning from patients about the experience of seeking and receiving care
- Informing strategic planning, policy development, resource allocation, and process adjustments
- Supporting a culture of continuous improvement
- Fostering patient and public trust
The validity of quality measures is compromised without transparency and input from key interest-holders. Therefore, we chose a stepwise and transparent process, published our findings in peer reviewed journals, and obtained input from relevant groups like researchers, providers, and administrators.
Preliminary measure development
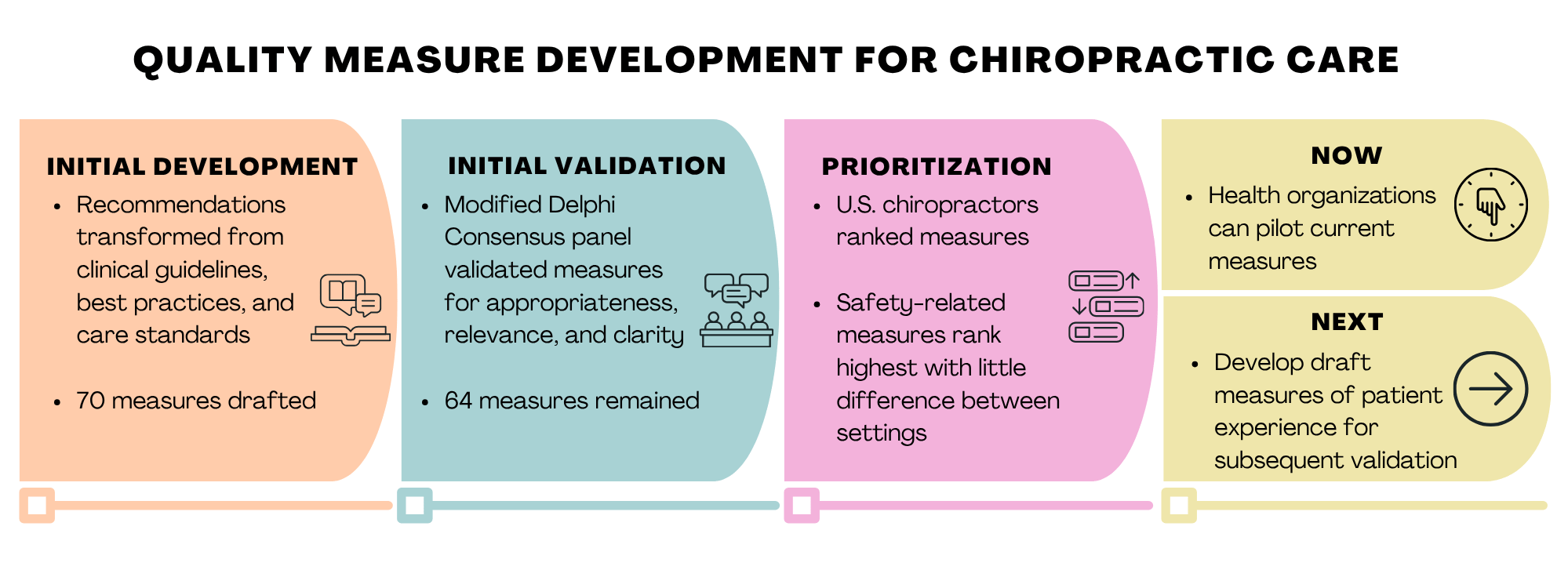
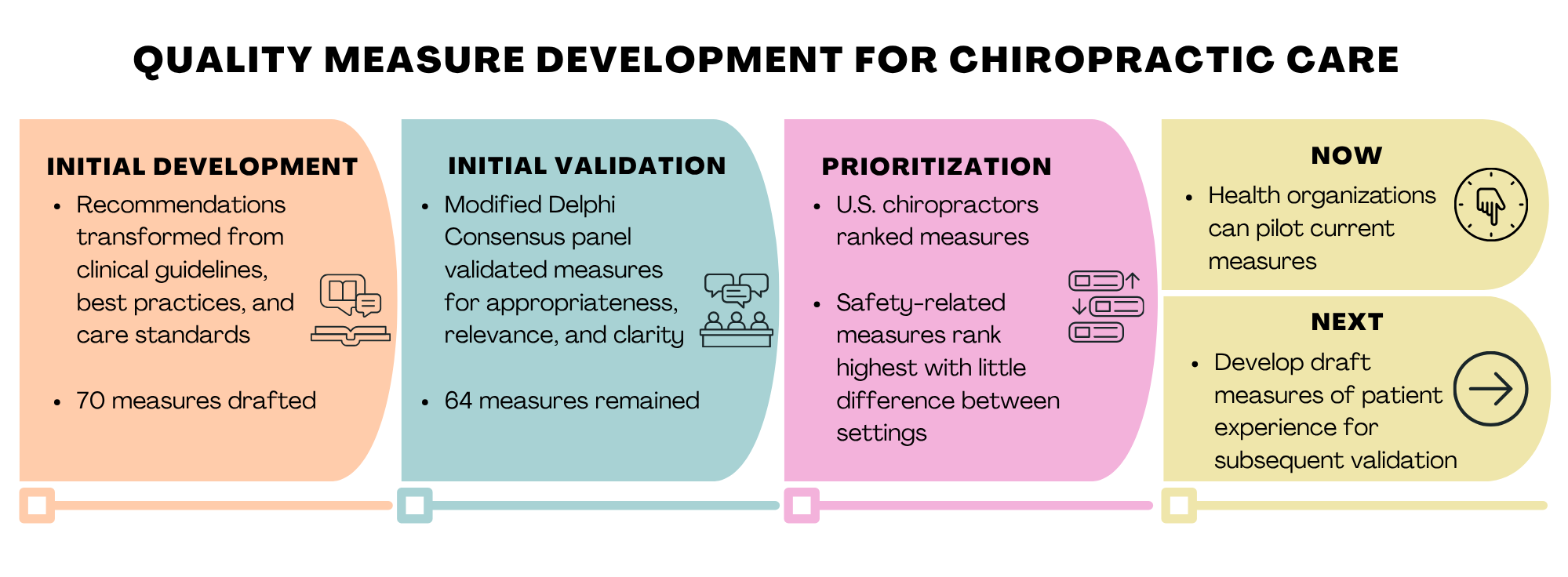
Following published guidance on quality measure development, we conducted a scoping review to obtain current clinical guidelines, best practices, and care standards relevant to chiropractic care. We then transformed recommendations from these sources into a draft set of 70 measures. Because the measures were supported by scientific literature and care standards, some validity was already present. But greater validation was needed, requiring input from an essential group of professionals.
Initial validation
The next step was drawing from the wisdom of a select group of practitioners and administrators to validate the appropriateness, relevance, and clarity of draft measures. We accomplished this by convening a Modified Delphi Consensus panel comprised of 46 clinical administrators from CCE-accredited institutions and residency programs, and practitioners and administrators in integrated care settings. Panelists were invited because they worked in settings which use quality measures or other administrative data to assess care for accreditation and other regulatory purposes. After the process was complete, 64 measures remained.
Prioritizing
Though more validation is needed, the current set of 64 measures is ready for pilot testing. But which ones are best to start with? The technical capacity to measure clinical processes varies across organizations. Some measures are highly feasible, others less so. And though quality is a universal concept, patient population needs and organizational characteristics can influence the relative importance and feasibility of some measures.
Therefore, to address questions about prioritization and feasibility while also engaging a wider interest-holder group, we conducted a U.S. national survey of chiropractors. We included practitioners in different geographic regions and practice environments to understand if certain setting features substantially changed how practitioners prioritized individual measures.
Two main findings came from this effort. The first was that despite differences in geography and practice characteristics, respondents ranked the importance and feasibility of measures with a high level of agreement. The second was that most of the highest ranked measures were directly related to safety. These findings are consistent with the idea that safe care is a fundamental component of quality. Without safety, the effectiveness of care greatly suffers and the value of other components of quality (equity, efficiency, patient-centeredness, and timeliness) is markedly reduced.
Where do we go from here?
Developing quality measures is a meaningless effort if they aren’t used. We encourage health organizations offering chiropractic services to begin piloting current measures. Implementation will be more successful if carefully planned, focusing first on the policies and infrastructure needed to support clinical processes and outcomes. What is learned from piloting a few measures can inform and enable broader use over time while also providing data on real-world feasibility and utility.
Measure development is an ongoing process. Currently, a critical element is missing – patient perspectives. Patient experience measures assess what patients experience during care, offering data to understand the effectiveness of policies and processes intended to support quality. These measures differ from satisfaction, which can be high even with poor quality care. Our team is developing patient experience measures as a next step.
Quality measures are not developed, validated, or implemented quickly. Once developed, they require continual review to support ongoing validity, alignment with advancing scientific evidence, and feasibility. The work requires a sustained long-term effort, reflecting a commitment to help ensure patients remain the primary focus and principal beneficiaries of care.
Follow the Topic
-
Chiropractic & Manual Therapies
This journal aims to improve patient care by publishing basic science, clinical and health services research that is relevant to chiropractors, manual therapists and related fields, including physical therapy, osteopathy, sports medicine, and rehabilitation.

Related Collections
With Collections, you can get published faster and increase your visibility.
Patient safety in chiropractic care and manual therapies
In May 2019, the World Health Organization (WHO) declared the protection of patients a global health priority through the resolution WHA 72.6, titled "Global action on patient safety." Yet, despite its recognized importance and advancements in technology and treatment, safety concerns in healthcare persist worldwide. By prioritizing high standards of care and vigilance, chiropractors may contribute to a safer healthcare system for all stakeholders, particularly patients.
This thematic series in Chiropractic & Manual Therapies (C&MT) is led by a diverse, international team of editors with a track record aligned in patient safety. Namely, senior epidemiologist Prof. Sidney Rubinstein, nurse scientist Dr. Stacie Salsbury, early career researcher Dr. Brian Coleman, whose expertise lies in implementation science and technology, and Prof Simon French, co-Editor-in-Chief at C&MT. Our editorial team invites authors to submit manuscripts focused on patient safety in chiropractic care. Submissions are encouraged in all formats accepted by the journal, including original research articles, systematic and scoping reviews, case reports, and study protocols. In addition, the series welcomes scholarly commentaries, debates, and letters to the editor that explore barriers and propose solutions to fostering and sustaining a strong global patient safety culture within chiropractic.
Submissions may include, but are not limited to, the following patient safety topics:
- Intervention or quality improvement studies of strategies to enhance the patient safety culture in chiropractic clinical settings, including individual practices, multi-specialty group practices, and hospital-based practices.
- Studies investigating perceptions of patient safety in chiropractic from key stakeholders, including patients, family members, chiropractors, and other healthcare professionals.
- The epidemiology of patient safety events where the occurrence and patterns of patient safety events relevant to chiropractic care are evaluated.
- Studies addressing patient safety considerations for special populations seeking or receiving chiropractic care, such as older adults or pregnant patients.
- Studies exploring the intersection of population characteristics and patient safety within chiropractic settings.
- Studies evaluating the effectiveness of curricular content and/or simulation-based training in enhancing chiropractic student and practitioner competency and proficiency in safety-related assessment and management.
Behind the Paper. From the authors, read about "Why We Mapped the State of Patient Safety Culture in Chiropractic Care."
Online conference. Following the end of this Call, we will organize an online-conference for all authors to present their work and discuss the importance of their findings
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Sep 15, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in