Why we analyzed editorial boards in Tropical Medicine journals—and what we found
Published in Biomedical Research

When we began exploring the power structures within tropical medicine journals, it wasn’t just an academic exercise—it was personal. As researchers from the Global South working in public health, we’ve often seen how the voices from regions most affected by tropical diseases are missing from the spaces where decisions about research priorities are made. Editorial boards, which determine what gets published and amplified, are one of those spaces. This paper grew out of a shared question: who holds the power to shape knowledge in tropical medicine, and what does that mean for equity in global health?
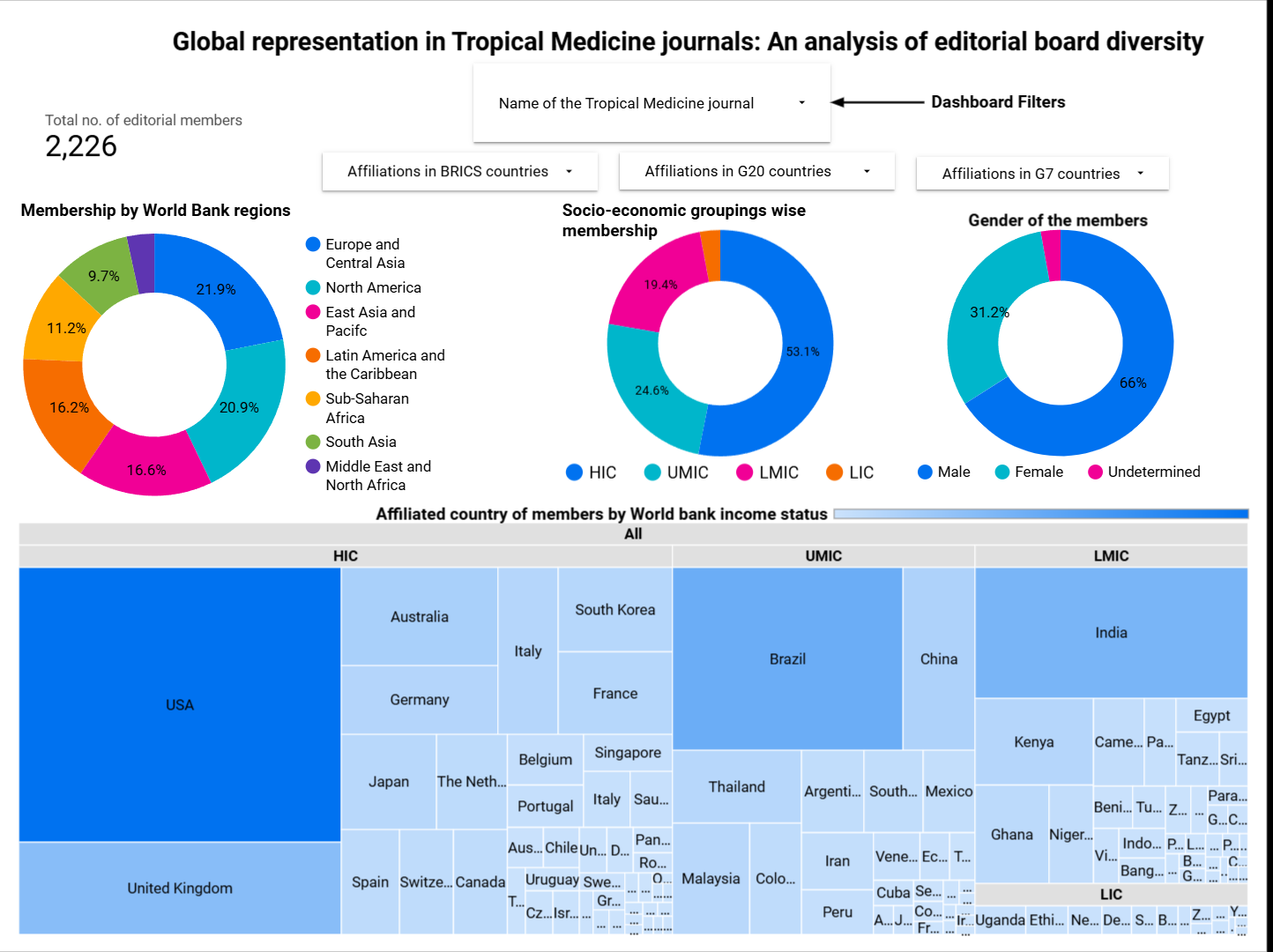
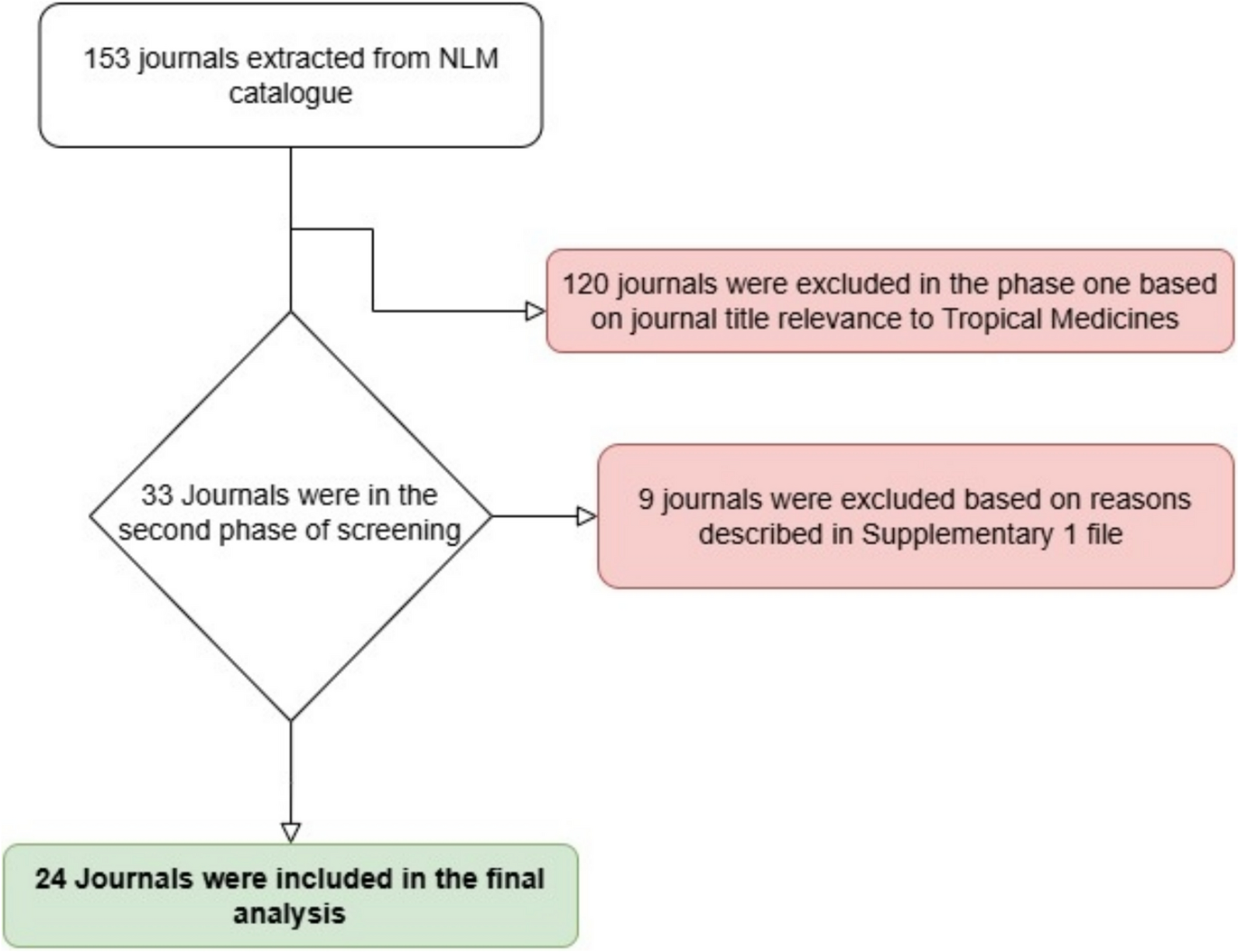
To investigate this, we systematically reviewed the editorial boards of 24 tropical medicine journals. Using publicly available data, we mapped the gender, geographic, economic, and political affiliations of 2,226 board members. The patterns we uncovered were troubling, though perhaps not surprising. About 66% (1,469) of editorial members were men, 31.2% (694) were women, and 2.8% (63) could not be determined. Over half (52.8%) were affiliated with high-income countries (HICs), while only 2.9% (64) were from low-income countries (LICs). Geopolitically, 40.3% (897) were based in G7 nations. In several journals, such as The American Journal of Tropical Medicine and Hygiene, over 85% of the board came from North America. The detailed findings are in interactive dashboard format . These boards are often responsible for deciding which research is “good science”—hardly reflect the diversity of the communities most impacted by tropical diseases.
This matters because editorial boards do more than select papers. They shape research agendas, signal whose knowledge counts, and reinforce or disrupt dominant narratives. The underrepresentation of scholars from LMICs, women, and non-Western regions perpetuates epistemic injustice: the systemic devaluation of certain types of knowledge, especially those rooted in lived experience, local context, or non-biomedical traditions. In many ways, the legacy of colonialism still lingers in global health publishing, not just in who gets to write, but in who gets to decide what’s worth reading.
We believe that this imbalance isn’t just an issue of fairness—it has ethical and practical consequences. If research continues to be shaped primarily by those far removed from the realities of tropical disease burden, we risk producing knowledge that is misaligned with community needs, or worse, ineffective in practice. To address this, we propose three steps. First, journals should commit to transparent and inclusive policies that actively prioritize diversity across gender, geography, and income levels. Second, mentorship programs should support researchers from LMICs in developing editorial and leadership skills. And third, recruitment processes must be redesigned to minimize biases and ensure fairer representation on editorial boards.
This work is a first step, not a final word. We hope it encourages other researchers, editors, and institutions to reflect on the invisible structures that shape what we publish and prioritize. Editorial boards are not just formalities; they are powerful spaces that can either reinforce global inequities or help dismantle them. It’s time to reimagine them through a decolonial lens—centering equity, valuing local expertise, and shifting power in global health publishing where it truly belongs.
Manish Barik is a public health researcher from India with degree in public health and a focus on health systems, policy, and epidemiology. Manish is passionate about translating evidence into practice and strengthening implementation in low- and middle-income countries, aiming to improve the responsiveness and inclusivity of global health systems.
Follow the Topic
-
Tropical Medicine and Health
Tropical Medicine and Health is an open access, peer-reviewed journal that publishes original research and reviews on all aspects of tropical medicine and global health. The journal welcomes clinical, epidemiological, laboratory and policy research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Exploring the New Frontier in Tropical Medicine with Computational Intelligence, AI, and IoT Integration for Healthcare
With the advancement of medical technology, the biomedical area brought about the big data age, which in turn gave rise to computational intelligent medicine, which is powered by technology. It is necessary to extract the useful information from these large biological data sets in order to advance precision medicine. A lot of time and human resources are needed to extract features from biomedical data using machine learning techniques, which often rely on feature engineering and expert domain knowledge. As a cutting-edge subfield of machine learning, deep learning differs from conventional methods in that it can automatically extract strong and sophisticated features from unprocessed data without the need for feature development.
Expanded Computational Intelligence (CI) assumptions are being used more and more to build robust digital applications that promote safety, quality, and efficacy in all areas of healthcare. Computational intelligence is based on technically inspired computational algorithms, and the primary components are genetic codes, neural networks, and fuzzy systems. Many techniques, fields, and natural processes have been used to characterize computational intelligence as a useful solution to real-world issues. Technological developments in recent years have opened up a wide range of applications for the Internet of Things (IoT), especially in the healthcare and medical sciences sectors. The use of data and different algorithms has led to the development of fascinating items such as healthcare robotics, precise sensors, smart healthcare, remote confirmation, and smart hospitals. In order to address health issues through Internet of Things applications, computational intelligence uses algorithms to create intelligent systems. Healthcare is one of the areas that computational intelligence is changing, and the growing sophistication of artificial intelligence is propelling significant industry expansion. The application of models like brain function modeling, algorithmic learning, game theory, and financial analysis, along with the growing market for computational intelligence, portends a new age of opportunities in the area.
Computational intelligence is capable of helping project a patient's risk of an infection, developing early alarms that can help medical professionals respond as quickly as possible. The use of computational intelligence to estimate infections in patients using physiological data as features. This special issue explores the use of computational intelligence in healthcare, which has greatly accelerated the digitization of health services. Computational intelligence allows computers to perform tasks that ordinarily require human intelligence, leading to significant breakthroughs in healthcare, including more effective drug discovery and better screening of patients for clinical trials.
We welcome papers on but not limited to:
• Health Care Forecasting for Different Illnesses via Computational Intelligence Methods
• A Strategy for applied smart health care informatics from the perspective of computational intelligence
• Using artificial intelligence to diagnose heart conditions automatically in healthcare systems
• Soft processing and computational intelligence implications for healthcare management economics
• An overview of the uses, difficulties, and operation of computational intelligence in healthcare
• Health care technology and the development of computational intelligence in contemporary medicine
• A structure utilizing computational intelligence approaches for decision support systems
• An Internet of Things strategy to combine wearable sensors and computational intelligence
• Healthcare applications of computational intelligence, with a focus on biological information science
• An Overview of Deep Computing and Computational Intelligence in Healthcare Informatics
• Methods and Uses of Computational Intelligence in Medical Evaluation and Choice Making.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being .
We are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or contact the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Oct 01, 2026
Clinical Questions in Tropical Medicine and Health
Tackling the management of febrile and non-febrile patients who cross country borders, is becoming a bigger and bigger challenge for physicians working in both high and low-middle income countries. Sharing clinical experiences, knowledge and skills is always interesting and helpful to clinicians working in different settings.
In this special issue of Tropical Medicine and Health, we call for case reports of infectious and non-infectious tropical diseases in returning travelers and people living in the disease endemic area. We ask that you first describe a short or long case presentation, secondly raise clinical questions, and then summarise the report with a discussion and take home message. We ask that your whole report is within 1200 words. This special issue welcomes case reports of common and less common infectious and non-infectious tropical diseases. We ask that convey information that helps lead to the diagnosis, including relevant pictures, and with clinical pearls that will help tropical medicine physicians in their daily practice. We also accept manuscript that are secondary publication of a case reports, already published in a local language.
Publishing Model: Open Access
Deadline: Feb 02, 2027
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in