PGS Singapore - Approval as Mainstream Clinical Service?
Published in Healthcare & Nursing, Social Sciences, and Genetics & Genomics
Please note:
-
The PGT-A technique has been given a red light rating in the United Kingdom, due to doubtful data on its effectiveness in improving IVF success rates.
-
Likewise, the American Society for Reproductive Medicine (ASRM) stated that the broad application of PGT-A on all IVF patients cannot be recommended due to doubtful results on improving live birth rates, and that its effectiveness in lowering the risk of miscarriages also remains unclear.
-
There are currently ongoing lawsuits against the PGT-A technique in the USA. The plaintiffs allege that they have not been properly informed about the various risks and limitations of the technique, and have been misled into discarding viable embryos, which have robbed them of their chances of parenthood.
-
The Australian fertility clinic Monash IVF agreed to compensate A$56 million to over 700 former patients for inaccurate and faulty genetic testing of IVF embryos, which led to the destruction of potentially viable ones.
Please also see the slide presentation video:
PGT-A on Trial: Groundbreaking Interview with the Lawyer Taking On the Fertility Industry
Currently, Preimplantation Genetic Testing - Aneuploidy (PGT-A) is not approved as a mainstream clinical service in Singapore by the Ministry of Health (MOH), unlike the case of PGT-M (monogenic disorders) and PGT-SR (chromosomal structural rearrangements). Instead, the clinical application of PGT-A in Singapore is restricted to a tightly controlled pilot clinical trial at public hospitals, where patients have to meet stringent criteria to qualify. These include being above 35 years of age, having suffered two or more recurrent implantation failures, or having experienced two or more pregnancy losses.
To date, the government-sponsored pilot clinical trial of PGT-A at public hospitals in Singapore has been reported to yield inconclusive results, with a rather high attrition rate due to withdrawal or cancellation of the procedure arising from various factors, such as failure to obtain blastocyst-stage embryos on day 5. As reported to the Singapore parliament in January 2024, 590 patients have been enrolled in the study, but only 195 patients had undergone PGT-A, of which 131 completed their embryo transfers. This has led to 70 pregnancies with 56 live births, and 5 ongoing pregnancies. It was recommended that more patients need to be recruited into the pilot trial for a robust evaluation of the clinical efficacy of PGT-A, before determining whether PGT-A can be approved as a mainstream clinical service.
Due to such tight restrictions on PGT-A in Singapore, many local infertility patients choose to travel abroad to access the procedure, with neighboring Malaysia being a preferred destination. In our present era of rapidly declining birth rates, whereby parents willingly invest more money, time and effort per child, PGT-A testing represents a lucrative market. Because most Singaporean patients traveling abroad for IVF treatment tend to be older women with a higher risk of having a baby with Down Syndrome, foreign fertility clinics can readily play on their fears to hard-sell this expensive accessory procedure.
A rather convincing sales pitch is that it would be wiser for IVF patients to spend a bit more on PGT-A, rather than risking the trauma of aborting a genetically abnormal fetus, or even worse, spending more money on the special education and health care needs of a Down Syndrome child. To further sweeten the deal, foreign IVF clinics often allow Singaporean patients to discreetly and covertly select the sex of their IVF embryo with PGT-A testing, even though non-medical sex selection for social reasons may in fact be banned by their local medical professional organization, such as in the case of Malaysia.
The PGT-A technique purportedly improves pregnancy success rates and reduces miscarriage risks among IVF patients by screening and weeding out IVF embryos with chromosomal abnormalities. However, evidence of its effectiveness in improving live birth rates is doubtful, especially for certain age groups.
Nevertheless, many Singaporean patients traveling abroad for IVF treatment are often ignorant that the PGT-A technique has been given a red light rating (indicating caution) in the United Kingdom, regarding its ability to improve IVF success rates. Moreover, the American Society for Reproductive Medicine (ASRM) stated that the broad application of PGT-A on all IVF patients cannot be recommended due to doubtful results on improving live birth rates, and that its effectiveness in lowering the risk of miscarriages also remains unclear.
Clinical trials involving hundreds of patients across multiple clinics in different countries have conclusively shown that PGT-A does not significantly enhance IVF success rates. Key studies include the 2018 ESTEEM trial and the 2019 STAR trial, both conducted in Western countries, along with a 2021 clinical study from China that was published in the highly reputable New England Journal of Medicine. Furthermore, an analysis of 133,494 IVF cycles in the Society for Assisted Reproductive Technology Clinical Outcome Reporting System database indicated that implementation of PGT-A in patients with late-stage embryos (blastocysts) available for transfer or screening is linked to a reduced cumulative live birth rate relative to conventional IVF. This negative correlation was notably more pronounced in individuals younger than 35 years, while no similar effect was observed in patients aged over 40.
Additionally, most Singaporean patients traveling abroad for IVF treatment are also unaware of ongoing class-action lawsuits against PGT-A in the United States, where it has been identified as the most glaring and widespread example of fraud within the IVF landscape. These lawsuits are underpinned by substantial evidence suggesting that PGT-A tests are often inaccurate and based on flawed assumptions, and that their effectiveness is often overstated, raising ethical and financial concerns for IVF patients.
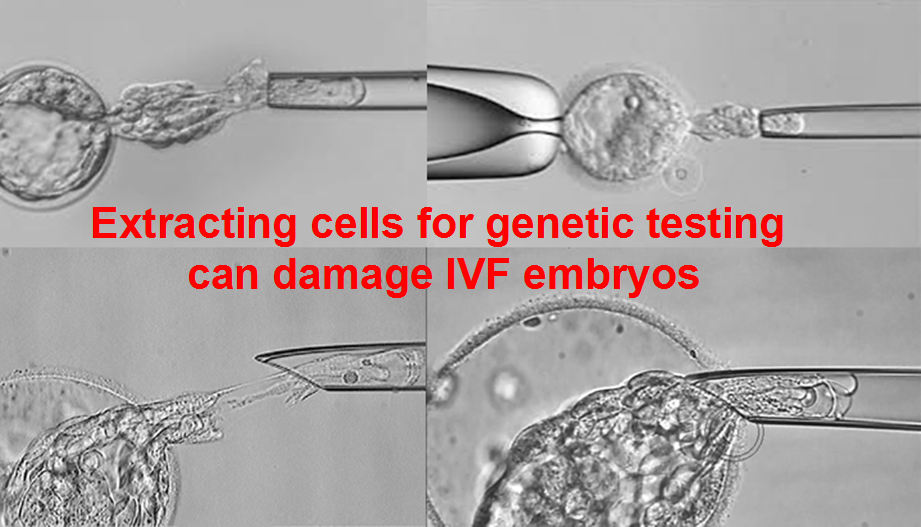
Very often, American fertility clinics offering PGT-A testing do not sufficiently disclose the inherent risks to patients, such as the potential for misdiagnosis and the risk of embryo damage due to the extraction of cells for genetic testing (biopsy). Although some published clinical studies have demonstrated that embryos are not harmed by the biopsy procedure, these results were often based on good-quality embryos from younger women.
Older women tend to produce fewer, lower-quality embryos that are more vulnerable to damage by biopsy. Moreover, the busier the IVF lab, the greater the risk of human error damaging the embryo during the delicate biopsy procedure. Although some published clinical studies have demonstrated that IVF embryos are not harmed by the biopsy procedure, these results were often based on good-quality embryos from younger women. Older women tend to produce fewer, lower-quality embryos that are more vulnerable to damage by biopsy. Moreover, the busier the IVF lab, the greater the risk of human error damaging the embryo during the delicate biopsy procedure.
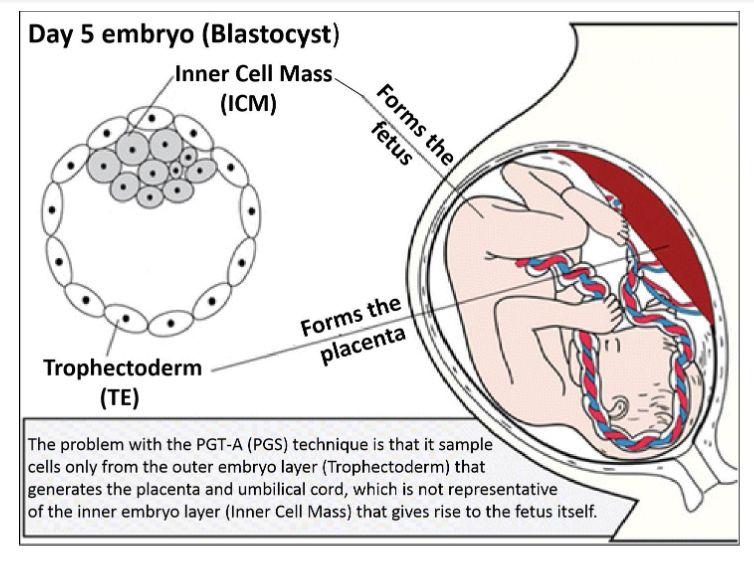
Because the biopsy process involves taking cells only from the outer embryo layer that forms the placenta and umbilical cord, but not the baby itself, this can sometimes yield inconclusive or misleading results, making treatment decisions complicated. Moreover, PGT-A may inadvertently reduce the chances of a successful pregnancy, as it often results in fewer embryos being available for transfer. Potentially viable embryos erroneously deemed to be ‘abnormal’ may be discarded, thus lowering overall IVF success rates.
The lawsuits, initiated by national class action law firm Berger Montague LLC, along with co-counsel Constable Law LLC and Justice Law Collaborative LLC, target multiple genetic testing companies, including CooperGenomics Inc., CooperSurgical Inc., The Cooper Companies Inc., Reproductive Genetic Innovations LLC, Progenesis Inc., and Natera Inc. These companies regularly advertise PGT-A as a genetic test for evaluating the normality of human IVF embryos by screening for chromosomal abnormalities.
In the USA, IVF patients are often encouraged to add on PGT-A as an additional screening test, which can cost several thousand dollars and is typically not covered by insurance. The complaints assert that the defendants have provided misleading information regarding the accuracy of PGT-A testing, thus making them complicit in consumer fraud and breach of warranty. To date, several large clinical trials have already demonstrated that PGT-A does not significantly improve IVF outcomes, and that it is unproven, unreliable, experimental, and inaccurate.
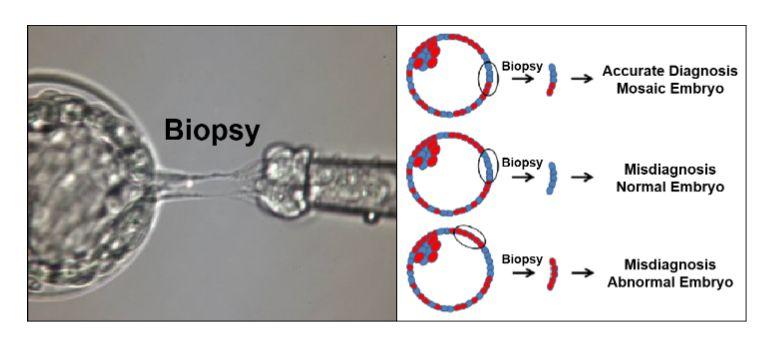
Such essential information was not disclosed to vulnerable patients charged with making critical decisions about which embryos to transfer based on the test results. This has potentially prevented patients from making fully informed decisions, raising ethical concerns regarding transparency and patient autonomy. The case also highlights that PGT-A testing often leads to false negatives, whereby mosaic embryos containing a mixture of genetically normal and abnormal cells, which can potentially give rise to a healthy baby, are mistakenly identified as unsuitable for transfer and are therefore discarded. This created emotional distress for patients who were previously unaware that viable embryos had been lost due to inaccurate testing, while also diminishing their opportunity for a successful pregnancy.
The plaintiffs thus seek to recover their out-of-pocket costs spent on PGT-A. Additionally, there are also statutory claims and other damages resulting from the defendants’ allegedly false and misleading promotion of PGT-A. Many former IVF patients claim that they would not have purchased the test if they had been provided with more accurate information regarding its effectiveness and potential risks, including misdiagnosis and embryo damage during biopsy.
In a similar lawsuit in Australia, the fertility giant Monash IVF has agreed to a payout of A$56 million to compensate 700 former IVF patients who had their viable embryos destroyed due to inaccurate genetic testing, which had robbed many of them of their chances of motherhood forever. This lawsuit highlighted the heartbreaking consequences that can result from reliance on flawed genetic testing procedures, leaving many patients with unresolved grief.
Despite the spate of unfavorable and doubtful results on PGT-A, there are sociocultural imperatives for Singapore to approve PGT-A as a mainstream clinical treatment, which should also be made readily available in the private healthcare sector. The rationale is that from the sociocultural perspective of some Singaporean patients, the benefits of PGT-A in preventing Down syndrome and other aneuploidies associated with older mothers (> 35 years old), together with averting abortion after prenatal testing; would far outweigh the various disadvantages and pitfalls of the procedure, such as misdiagnosis due to chromosomal mosaicism, possible reduction in live birth rates due to risks of biopsy damaging the embryo, and overall lack of cost-effectiveness. Various sociocultural imperatives would favor the uptake of PGT-A in Singapore, which will thus be examined.
First, Singapore has undergone a major demographic shift in the past two decades, with an increasing trend of late motherhood and a drastic reduction in fertility rates. Since 2017, the total fertility rate (TFR), defined as the average number of children that a woman will have in her lifetime, has been consistently below 1.2. In 2022, Singapore’s resident TFR hit an all-time low of 1.05, dipping below the previous records of 1.1 in 2020 and 1.12 in 2021. The new generation of better-educated Singaporean women is well aware that the increasing trend of late motherhood in Singapore is closely associated with higher risks of Down syndrome and other chromosomal abnormalities. Some IVF patients among them would rather spend extra money on expensive PGT-A to avoid the risks of abortion upon positive diagnosis after prenatal testing. Although medical advances have made abortion a relatively safe procedure, vigorous campaigning and publicity stunts by pro-life activists have widely portrayed the procedure as being highly risky, painful and harmful to health, resulting in many women being highly fearful of the procedure. Moreover, a drastic reduction in fertility rates, leading to most Singaporean women having only one child, would motivate them to invest more in their single offspring, including doing highly expensive PGT-A to eliminate the possibility of Down syndrome and other aneuploidies. In 2022, it was reported that the costs of PGT testing in Singapore ranged from SGD$ 11,000 to SGD$ 31,000 (approximately USD$ 8,000 to USD$ 23,000). The costs of the procedure are not covered by insurance, but residents can receive up to a 75% fee subsidy from the Singapore government.
Second, although Singaporean society has increasingly become more secular in recent years, the majority of the population still hold religious beliefs and are significantly more religious compared to many Western societies. Higher levels of religiosity would equate to greater aversion to abortion, which is unanimously considered to be immoral by all major religious faiths in Singapore. Presumably, some Singaporean patients with strong religious beliefs would be motivated to avoid abortion at all costs, so as not to offend their religious beliefs and hurt their conscience. Adding highly expensive PGT-A to IVF treatment cycles would thus avert the risks of abortion for some older women (> 35 years old) with strong religious beliefs.
Third, Down syndrome and other aneuploidies are heavily stigmatized and scorned in Asian Confucian societies such as Singapore. This contrasts sharply with liberal Western values that stress the need to promote the rights of disabled individuals and accommodate their special needs. In the predominantly Chinese culture of Singapore, individuals with Down syndrome and other aneuploidies are often scorned and despised as a burden on society, as well as considered a shame and embarrassment to their families. This would thus motivate some older women (> 35 years old) undergoing IVF to use all means at their disposal to avoid Down syndrome and other aneuploidies, even if that means adding highly expensive PGT-A to their IVF treatment. In the mindset of some prospective parents in Singapore, it would be wiser to spend extra money on expensive PGT-A to ensure the birth of a normal and healthy child, rather than risking abortion or spending more money on the healthcare and upbringing of a disabled child. Hence in this context, PGT-A would play a key role in reassuring IVF patients, particularly older women (> 35 years old), that Down syndrome and other aneuploidies would be prevented and the risks of abortion averted, thus giving them much-needed peace of mind during the stressful IVF procedure.
Hence, based on these aforementioned sociocultural imperatives, the Ministry of Health in Singapore should allow local IVF patients the option of adding on PGT-A, despite the current controversy on its therapeutic value and cost-effectiveness. It is anticipated that some older women (> 35 years old) would be willing to spend the extra money and incur the risks associated with the procedure, just for the sake of preventing Down syndrome and other aneuploidies, as well as for avoiding the risks of abortion. An appropriate analogy here would be prenatal testing techniques such as amniocentesis and chorionic villus biopsy (CVB). The risks associated with these techniques are well-known and there are no therapeutic benefits in improving live birth rates.
Yet, it is anticipated that some patients would still be willing to incur the risks and pay for these diagnostic procedures. In this light, PGT-A should be more correctly viewed as a diagnostic cum preventive procedure that incurs some degree of risks, rather than as a therapeutic procedure to enhance IVF success rates. In any case, there should be compulsory counseling for all patients considering PGT-A by a qualified genetic counselor to ensure that they are well aware of the various disadvantages and pitfalls of the procedure. These include misdiagnosis due to chromosomal mosaicism, possible reduction in live birth rates due to risks of biopsy damaging the embryo, and overall lack of cost-effectiveness. Additionally, patients must also be informed that mosaic embryos have the potential to self-correct and give rise to a normal, healthy baby, so that the discarding of mosaic embryos will reduce their cumulative chances of reproductive success. By mandating comprehensive and rigorous genetic counseling, the Singapore Ministry of Health can ensure better patient awareness of the various pros and cons of the PGT-A procedure. In particular, it is important to counter aggressive advertising by private IVF clinics that misrepresent PGT-A as a therapeutic procedure that has beneficial effects in improving IVF success rates, because the latest uncertain and ambiguous clinical data have cast much doubt on such claims. As mentioned earlier, patients should be strongly advised to view PGT-A more accurately as a diagnostic cum preventive procedure that carries some degree of risks, similar to amniocentesis and CVB.
Please refer to the following articles:
Malaysian IVF Patients Must Be Warned About US Lawsuits Involving PGT-A (PGS)
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in