Anti-CD38 Monoclonal Antibody Therapy in Myeloma: New Considerations for Timing and Sequencing
Published in Cancer

Multiple myeloma (MM), a malignancy of plasma cells, is characterized by abnormal overproduction of monoclonal immunoglobulin. A permissive microenvironment in bone marrow and immune dysregulation are pivotal to myeloma cell growth, proliferation, and migration, as well as clinical manifestation and drug resistance in MM.1,2 Therapies that modulate the immune system, including immunomodulatory drugs (IMiDs) and monoclonal antibodies (mAbs), are the current mainstay of MM treatment. The transformative impact of these therapies is reflected in the doubling of MM survival over the past 2 decades.3–5 Despite this progress, MM remains a therapeutic challenge. Moreover, as new combinations are increasingly used in earlier lines, patients with relapsed/refractory MM (RRMM) develop resistance to multiple drugs, requiring innovative approaches for management.6
To date, 2 mAbs that target the transmembrane glycoprotein ectoenzyme CD38 – daratumumab and isatuximab – are approved for use in MM.5 These mAbs, which demonstrate activity as single agents and in combination with IMiDs or proteasome inhibitors (PIs), have proven remarkably useful in treating RRMM. However, as with other drug classes, patients develop anti-CD38-mAb–refractory MM, which is associated with a poor prognosis, even in patients who remain responsive to IMiD or PI therapy.7 In addition to novel classes of agents, retreatment with anti-CD38-directed therapy in patients with RRMM refractory to anti-CD38 mAb treatment might be an option.
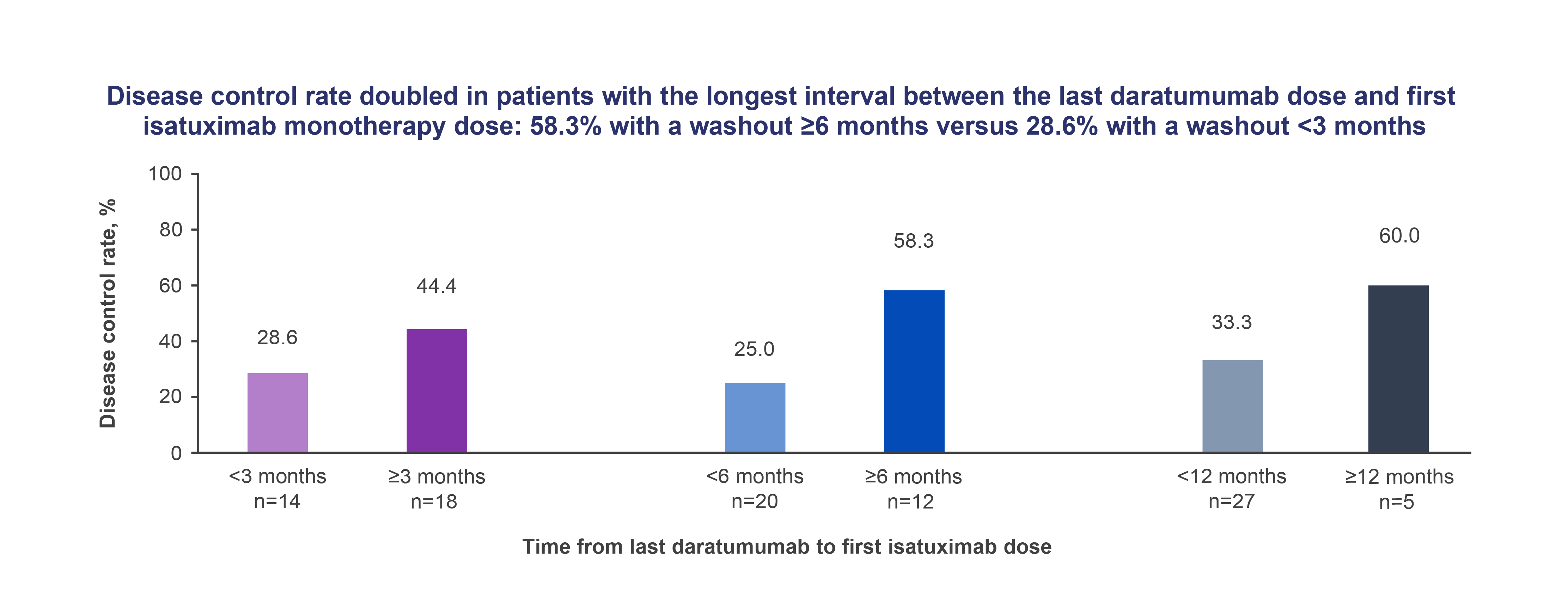
The question of retreatment with the same/different mAbs in anti-CD38-mAb–refractory disease is unresolved, although real-world and retrospective analyses have shown responses in some daratumumab-refractory patients subsequently treated with isatuximab or daratumumab, in combination with pomalidomide and dexamethasone.8,9 Our Phase 1/2 clinical study, which explores isatuximab safety and efficacy in daratumumab-refractory patients (over 50% received daratumumab combination therapy), provides some insights into this data gap. In our cohort of 32 heavily pretreated patients (median 7 prior lines) with daratumumab-refractory MM, the disease control rate (DCR) was 37.5%. Notably, the DCR was higher in patients who received isatuximab over longer intervals after their last daratumumab dose, 60%, 58.3%, and 28.6% in those with ≥12, ≥6, and <3 months of daratumumab washout, respectively (Figure). Isatuximab treatment improved median overall survival over historical data for CD38-mAb–refractory patients (10.7 vs 8.67 months).

While both daratumumab and isatuximab target CD38, isatuximab induces MM apoptosis independent of effector cells and cross-linking agents.10 It is a more potent inhibitor of CD38 enzymatic activity, thereby reducing adenosine in the bone marrow microenvironment, making it less hospitable for myeloma cells and more conducive to anti-cancer immune responses.10 Isatuximab will likely be used in earlier lines as well as in combination with other agents, based on currently approved indications. However, our data suggest clinical potential and optimal timing of isatuximab monotherapy in MM refractory to daratumumab combinations in advanced MM patients who do not have many treatment options at this time of their disease. Additional studies are needed to reveal the complete picture of the depth and duration of responses. As the MM therapeutic arsenal continues to expand and gain complexity, further clinical trials are also needed to clarify the optimal timing, sequencing, and choice of anti-CD38 mAb monotherapy or combination regimens in anti-CD38-mAb–refractory MM, providing a roadmap for maximizing the therapeutic returns in RRMM.
References
- Romano A, Conticello C, Cavalli M, et al. Immunological dysregulation in multiple myeloma microenvironment. BioMed Res Int. 2014;2014. doi:10.1155/2014/198539
- Lopes R, Ferreira BV, Caetano J, Barahona F, Carneiro EA, João C. Boosting immunity against multiple myeloma. Cancers. 2021;13(6). doi:10.3390/cancers13061221
- Nandakumar B, Binder M, Dispenzieri A, et al. Continued improvement in survival in multiple myeloma (MM) including high-risk patients. J Clin Oncol. 2019;37(15_suppl):8039-8039. doi:10.1200/JCO.2019.37.15_suppl.8039
- Gulla A, Anderson KC. Multiple myeloma: the (r)evolution of current therapy and a glance into future. Haematologica. 2020;105(10):2358-2367. doi:10.3324/haematol.2020.247015
- Radocha J, van de Donk NWCJ, Weisel K. Monoclonal antibodies and antibody drug conjugates in multiple myeloma. Cancers. 2021;13(7). doi:10.3390/cancers13071571
- Rajkumar SV, Kumar S. Multiple myeloma current treatment algorithms. Blood Cancer J. 2020;10(9):94. doi:10.1038/s41408-020-00359-2
- Gandhi UH, Cornell RF, Lakshman A, et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia. 2019;33(9):2266-2275. doi:10.1038/s41375-019-0435-7
- Becnel MR, Horowitz SB, Thomas SK, Iyer SP. Descriptive analysis of isatuximab use following prior daratumumab in patients with relapsed/refractory multiple myeloma. Presented at: 62nd ASH Annual Meeting and Exposition; December 5-8, 2020. https://ash.confex.com/ash/2020/webprogram/Paper140526.html
- Nooka AK, Joseph NS, Kaufman JL, et al. Clinical efficacy of daratumumab, pomalidomide, and dexamethasone in patients with relapsed or refractory myeloma: Utility of re-treatment with daratumumab among refractory patients. Cancer. 2019;125(17):2991-3000. doi:10.1002/cncr.32178
- Martin TG, Corzo K, Chiron M, et al. Therapeutic opportunities with pharmacological inhibition of CD38 with isatuximab. Cells. 2019;8(12). doi:10.3390/cells8121522
Follow the Topic
-
Blood Cancer Journal
This journal seeks to publish articles of the highest quality related to hematologic malignancies and related disorders.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in