When someone is living with depression, finding a treatment that actually helps can take time, often through painful trial and error. For some people, that process is even harder: after trying more than one antidepressant at an appropriate dose and duration, symptoms still don’t meaningfully improve. Clinicians call this treatment-resistant depression (TRD), and for patients and families it can feel like running out of options.
We wanted to ask a simple, but surprisingly tricky, question: can you model TRD in a mouse?
TRD in humans is often defined as failure to respond to two adequate antidepressant trials. But what does “adequate” mean in a mouse? In people, treatment can last months. In rodents, depressive-like behaviors induced by chronic social defeat stress (CSDS) may not persist long enough to realistically model that timeline. The biology and the clock don’t align neatly.
So we had to make a decision: do we try to replicate the clinical definition exactly, or do we model the core concept of treatment resistance?
We chose the latter.
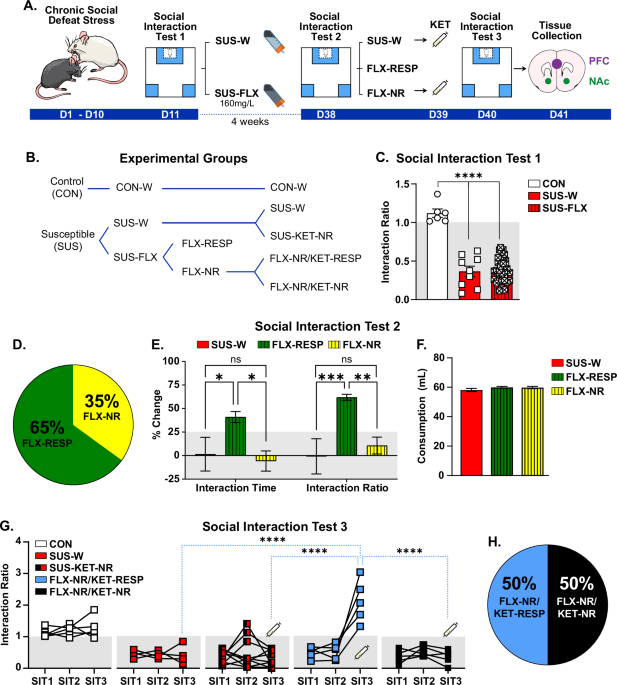
After CSDS, we identified susceptible mice using the social interaction test. We then treated one group with fluoxetine (FLX) for 30 days, long enough to approximate chronic SSRI exposure in rodents. About 65% responded. Roughly 35% did not. That number caught our attention: it mirrors the proportion of patients who do not benefit from first-line antidepressant treatment.
But here’s where the story became interesting. We next gave an acute injection of ketamine to all of the fluoxetine non-responders. In parallel, we gave ketamine to a separate group of susceptible mice that had never received fluoxetine. The results surprised us. None of the mice that received ketamine as a first-line treatment responded at the 4-week post-stress time point. But 50% of the fluoxetine non-responders did respond to ketamine.
Ketamine has repeatedly been shown to reverse stress-induced behavioral deficits in mice when given within two weeks after CSDS. By four weeks, that window may close. We expected ketamine to fail across the board at that later time point.
It didn’t.
Fluoxetine exposure, even when behaviorally ineffective, appeared to “prime” the system to respond to ketamine. That raised a new possibility: perhaps treatment resistance is not simply the absence of drug effect. Perhaps antidepressants still induce molecular changes in non-responders—changes that alter how the brain responds to subsequent treatments.
To explore that idea, we performed bulk RNA sequencing. We wanted to know whether mice that fail to respond to antidepressants share a molecular signature. Are non-responders biologically similar to one another? Or is “treatment resistance” simply noise?
What we found suggests that non-response is not random. There is a transcriptional signature associated with treatment resistance, a pattern that distinguishes mice that fail multiple treatments from those that respond.
Of course, we are cautious. This is still a rodent model. We cannot replicate the full clinical trajectory of TRD, with months-long treatments and washout periods. Single housing our mice is necessary to track fluoxetine consumption, and it adds another layer of complexity because it can be viewed as an additional stressor.
But perhaps modeling TRD does not require perfect replication of the human definition. Perhaps it requires capturing the biological logic: that some individuals fail first-line treatment, some respond to second-line therapies, and that these outcomes reflect underlying molecular differences.
This study began with skepticism: can we really model treatment resistance in rodents? It ended with a more nuanced answer.
Maybe not perfectly.
But perhaps closely enough to start asking the right biological questions.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in