Cancer risk in kidney transplant patients in Scotland: a national registry analysis
Published in Cancer, General & Internal Medicine, and Surgery
Chronic kidney disease is the reduced ability of the kidneys to remove waste products from the body. It affects 1.8 million people in the UK, and £1 of every £77 spent by the National Health Service is for the treatment of kidney disease and its associated complications. At the severe end of the spectrum, people develop kidney failure and may need dialysis or a kidney transplant. Kidney transplantation is associated with improved survival compared to dialysis, improved quality of life and cost effectiveness. It is therefore the recommended treatment for most people with kidney failure.
To prevent the body recognising a kidney transplant as ‘foreign’, which can lead to activation of the immune system and rejection of the transplant, people receive immune suppression medication. Whilst this is needed to maintain function of a kidney transplant, it comes with an increased risk of infections and cancer. In the UK, cancer is the third leading cause of death in kidney transplant recipients. To help guide counselling of patients before transplantation, it is important to how the cancer risk compares to that of someone not needing immune suppression, which cancers are most common so people can be monitored for these, and which patients are at the highest risk of cancer development. This is particularly relevant as the number of older people receiving a kidney transplant is increasing, and there have been changes to immune suppression practice since this was previously studied.
In this study we linked data from the Scottish Renal Registry, Scottish Cancer Registry, national hospitalisation records and national records for death to answer these questions. We looked at all kidney transplant recipients in Scotland who received their first kidney transplant between 1st January 1997 and 31st December 2021.
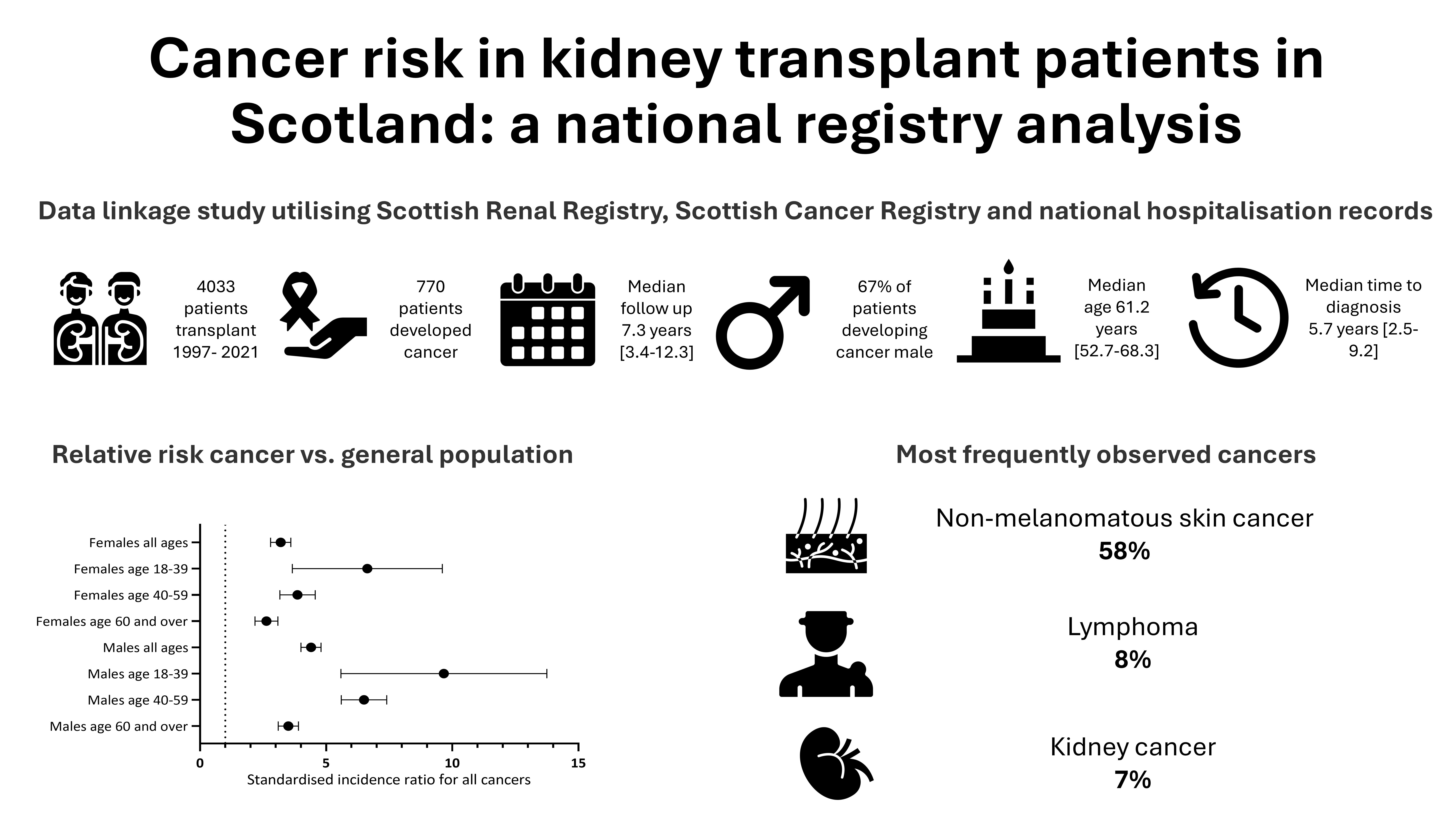
Overall 4033 patients were transplanted and had their follow up in Scotland over this time, of whom 770 patients (19%) developed cancer at a median age of 61.2 years. Two thirds of those developing cancer were male and the median time between transplant and cancer diagnosis was 5.7 years.
The most frequently observed cancers were different in transplant patients compared to the general population. Skin cancers (basal cell and squamous cell carcinomas), lymphoma and kidney cancers were the most frequently observed, followed by the most common cancers in the general population: lung, breast and prostate cancer. The cancer stage at diagnosis was similar between transplant recipients and the general population, aside from bladder cancer where a greater proportion of transplant recipients presented with advanced disease.
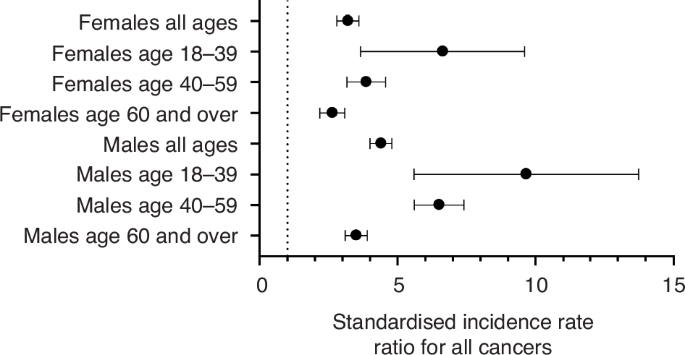
When comparing the risk of all cancers in transplant recipients to the general population, we found that younger transplant recipients below 40 years of age had a higher relative risk of cancer than older transplant recipients. However as cancer is more common generally in older individuals, the absolute risk of cancer remained greatest for older transplant recipients aged over 60. Men had higher absolute and relative risks of cancer than women. The relative increased risk of cancer was greatest for non-melanoma skin cancers, lymphoma, kidney and bladder cancer.
In the UK, cancer screening pathways exist for colorectal, breast and cervical cancer. When examining how many cancers were detected via screening routes, the proportion was similar between transplant recipients and the general population.
Finally, what other risk factors are there for cancer development? Being older, of male sex, having a history of cancer before transplantation, and having a longer history of kidney failure were seen to associate with cancer. We didn’t have information on all the potential risk factors however e.g. type and dose of different immune suppression medications, viral infections, how well matched the kidney was, and smoking history or sun exposure.
How could these results help? They will aid the counselling of transplant recipients on what their risk of cancer might be with a transplant, and for doctors highlights the most frequent cancers to be aware of. Even in Scotland, with lower UV exposure than many other parts of the world, skin cancers remained the most frequently observed cancer. Although the relative risk of cancer is highest in younger transplant recipients the absolute risk is greatest in older individuals and highlights the potential rationale for age-adjusted immune suppression protocols. Further the increased risk of cancer in men should be noted. The reasons for this aren’t fully understood, but making sure patients receive appropriate counselling on risk behaviours e.g. skin protection is clearly important as well as considering if there is capacity for skin surveillance clinics for transplant recipients. Whilst the results here cannot inform screening policies, which need to consider relative costs and benefits and impact on patient outcomes, they highlight to doctors looking after transplant recipients the importance of remaining vigilant to relevant signs and symptoms that could point towards an underlying diagnosis.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in