Definite Lyme Neuroborreliosis Despite Negative Antibody Index: Expanding the Diagnostic Framework
Published in Neuroscience and Biomedical Research
Explore the Research
Definite neuroborreliosis with atypical antibody-profiles: a case report
Case summary
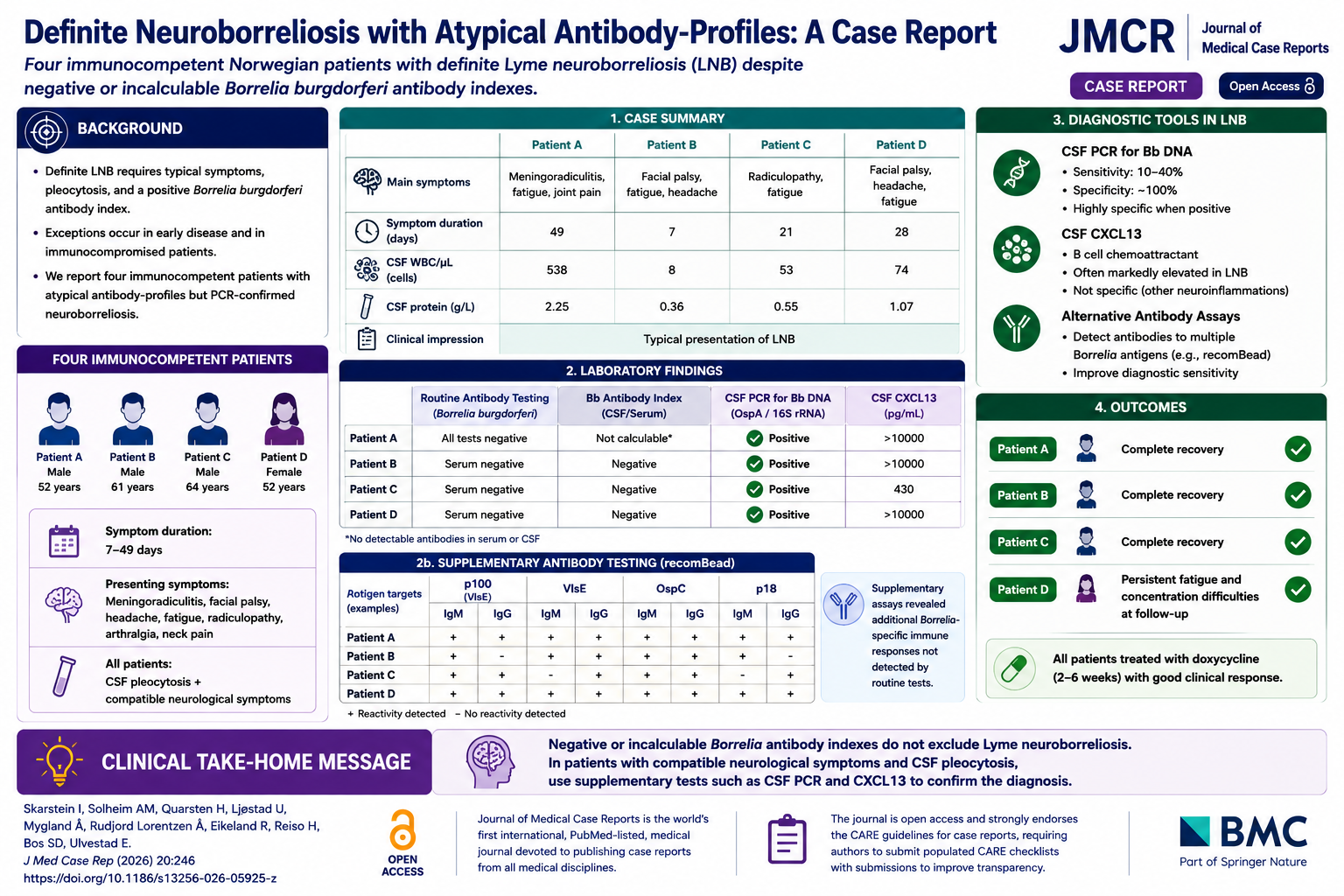
In this report, Skarstein and colleagues describe four Norwegian immunocompetent patients with clinical syndromes highly suggestive of Lyme neuroborreliosis (LNB) despite negative or incalculable Borrelia burgdorferi antibody indexes.
The patients—three men aged 52, 61, and 64 years and one 52-year-old woman—presented with combinations of painful meningoradiculitis, facial palsy, headache, fatigue, neck pain, arthralgia, and radiculopathy. Symptom duration ranged from 7 to 49 days. Cerebrospinal fluid (CSF) analysis demonstrated pleocytosis in all cases, with white blood cell counts ranging from 8 to 538 cells/µL.
Despite typical neurological presentations, routine serologic testing failed to establish definitive LNB. One patient had no detectable antibodies in serum or CSF, while others demonstrated discordant antibody patterns or negative antibody indexes. However, all four patients had positive CSF PCR for Borrelia burgdorferi DNA targeting the OspA and/or 16S rRNA genes, confirming the diagnosis.
Additional supportive biomarkers further strengthened the diagnosis. CSF CXCL13 levels were markedly elevated in all patients, frequently exceeding 1000 pg/mL. Supplementary recombinant antigen assays (recomBead) identified additional Borrelia-specific immune responses not detected by routine clinical testing. Tables 1 and 2 on page 3 demonstrate the atypical antibody profiles and positive PCR findings across all four patients.
All patients were treated with oral doxycycline for 2–6 weeks and demonstrated favorable clinical outcomes. Three patients experienced complete neurological recovery, while one reported persistent fatigue and concentration difficulties at longer-term follow-up.
The authors emphasize that negative routine antibody testing should not exclude LNB when clinical suspicion and CSF inflammation are strongly suggestive. Instead, supplementary testing—including CSF PCR, CXCL13 analysis, and expanded antibody assays—may be essential for confirming diagnosis in atypical presentations.
Why this case matters
- Challenges reliance on antibody index alone for diagnosing LNB
- Demonstrates PCR-confirmed neuroborreliosis despite negative routine serology
- Highlights the diagnostic value of CSF CXCL13 and supplementary antibody assays
- Reinforces that immunocompetent patients may still exhibit atypical immune responses
- Supports broader diagnostic frameworks in neurologically compatible cases
Clinical Take-Home Message
Negative or incalculable Borrelia antibody indexes do not exclude Lyme neuroborreliosis; in patients with compatible neurological symptoms and CSF pleocytosis, supplementary testing with CSF PCR and CXCL13 can be critical for establishing the diagnosis.
Question
Which finding definitively confirmed Lyme neuroborreliosis in all four patients despite atypical antibody profiles?
A. Elevated CSF protein
B. Positive MRI findings
C. Positive CSF PCR for Borrelia burgdorferi DNA
D. Presence of erythema migrans
Correct answer: C. Positive CSF PCR for Borrelia burgdorferi DNA
Explanation:
All four patients had atypical or negative antibody index findings, but CSF PCR targeting Borrelia burgdorferi DNA confirmed definite Lyme neuroborreliosis. Elevated CXCL13 levels and supplementary antibody assays provided additional supportive evidence.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in