JMCR: Clinical Reasoning From Case Reports
Published in Neuroscience and Biomedical Research
Explore the Research
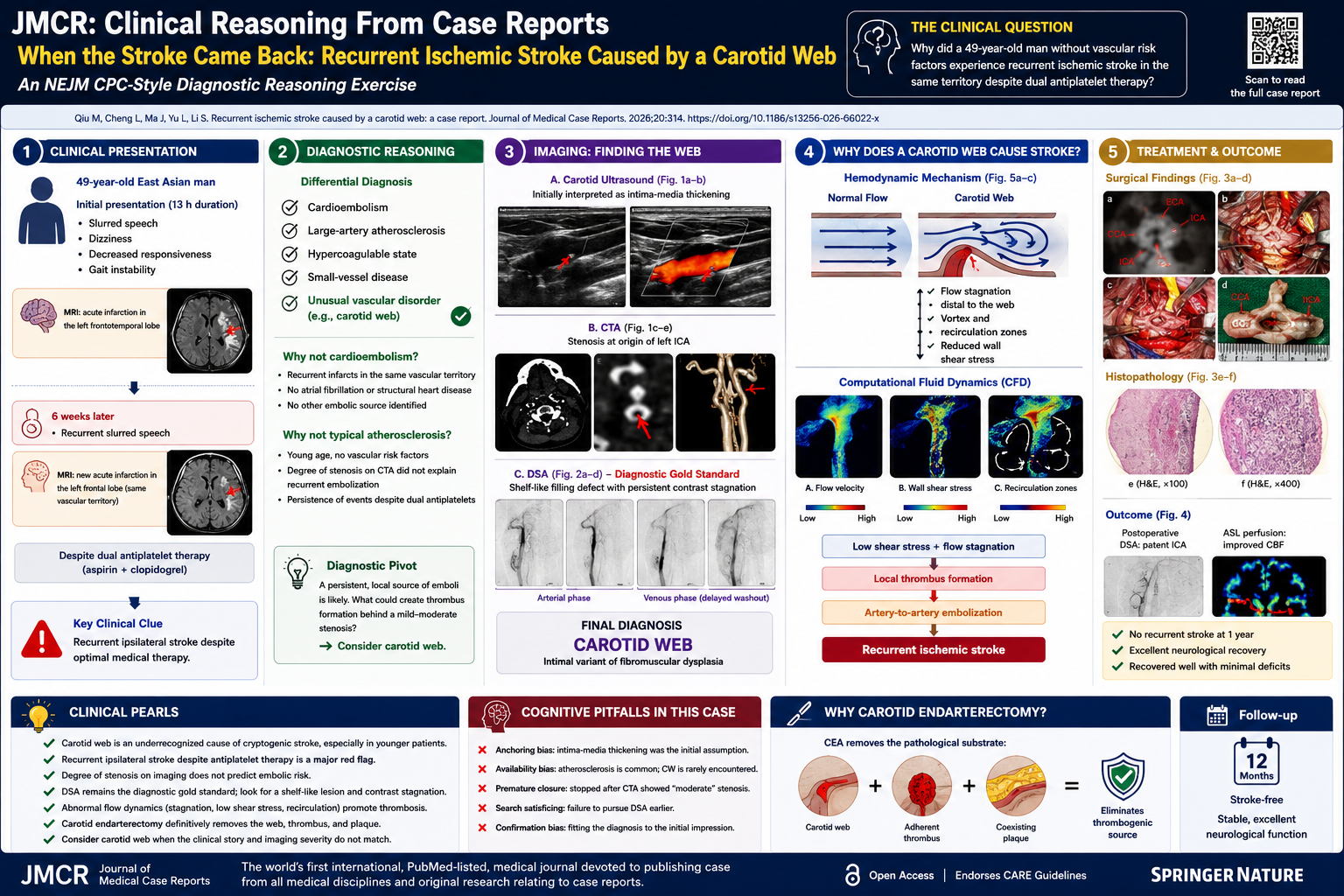
Recurrent ischemic stroke caused by a carotid web: a case report
Presentation of Case
A 49-year-old East Asian man presented to the hospital with a 13-hour history of slurred speech, dizziness, decreased responsiveness, and gait instability.
Brain magnetic resonance imaging demonstrated an acute infarction involving the left frontotemporal region. He was treated with aspirin, clopidogrel, Ginkgo biloba extract, and dl-3-n-butylphthalide, with stabilization of symptoms. Approximately six weeks later, however, he experienced recurrent slurred speech and was readmitted.
Repeat MRI revealed a new acute infarction involving the left frontal lobe within the same vascular territory. Arterial spin-labeling perfusion imaging demonstrated reduced cerebral blood flow throughout the left frontotemporal region. Carotid ultrasonography identified a hyperechoic abnormality at the origin of the left internal carotid artery, interpreted as intima-media thickening. Computed tomography angiography demonstrated localized stenosis of the proximal left internal carotid artery.
Routine laboratory studies, including blood counts, metabolic testing, coagulation studies, cardiac biomarkers, renal function, and hepatic function, were unremarkable.
The patient had no history of hypertension, diabetes mellitus, dyslipidemia, atrial fibrillation, smoking, or prior cerebrovascular disease.
What is the differential diagnosis?
Initial Differential Diagnosis
At first glance, this appears to be a relatively straightforward case of recurrent ischemic stroke. However, recurrent stroke occurring over a six-week interval despite dual antiplatelet therapy immediately suggests that an important component of the mechanism has not yet been identified.
The central question is not whether the patient has experienced ischemic strokes. The imaging establishes that diagnosis.
The critical question is:
Why is a 49-year-old man without major vascular risk factors continuing to suffer recurrent infarction despite contemporary secondary stroke prevention?
The differential diagnosis can be organized into five major categories:
- Cardioembolism
- Large artery atherosclerotic disease
- Small vessel disease
- Hypercoagulable disorders
- Unusual vascular disorders
Is This Cardioembolism?
Cardioembolism is among the most common causes of recurrent ischemic stroke.
Potential mechanisms include:
- Atrial fibrillation
- Left ventricular thrombus
- Patent foramen ovale
- Valvular disease
- Infective endocarditis
- Atrial cardiopathy
However, several aspects of the case argue against a cardioembolic source.
The recurrent infarctions occurred in the same vascular territory. Cardioembolic strokes often involve different arterial distributions over time because emboli may travel to any intracranial circulation.
Furthermore, no cardiac abnormalities were identified during the diagnostic evaluation.
Although cardioembolism cannot initially be excluded, the pattern increasingly suggests a local arterial source.
Is This Large-Artery Atherosclerosis?
The CTA demonstrated stenosis involving the proximal internal carotid artery.
At first glance, this appears to provide a straightforward explanation.
Yet several inconsistencies emerge.
The patient lacks conventional risk factors. More importantly, the degree of stenosis appears insufficient to explain recurrent embolic events despite aggressive medical therapy.
This discrepancy should immediately prompt caution.
One of the most common cognitive errors in vascular neurology is assuming that every carotid abnormality is atherosclerotic.
The clinician must ask:
Does the imaging abnormality adequately explain the clinical severity?
In this case, the answer appears to be no.
Neuroanatomic Localization
Both infarctions involved the left frontotemporal circulation.
This localization immediately implicates:
- Left internal carotid artery
- Left middle cerebral artery
- Less likely, the proximal anterior cerebral circulation
The recurrent involvement of the same vascular territory strongly suggests a persistent ipsilateral embolic source.
Small vessel disease becomes highly unlikely because lacunar infarctions generally occur within deep perforator territories and rarely recur repeatedly within the same cortical distribution.
The localization therefore points toward a lesion within the extracranial or proximal intracranial arterial circulation.
The Diagnostic Pivot
The most important clue in this case is not the stenosis.
It is the recurrence.
Atherosclerotic lesions primarily threaten patients through progressive narrowing or plaque rupture.
This lesion behaved differently.
Despite medical therapy, embolization continued.
Such behavior suggests a lesion whose primary danger is thrombogenesis rather than stenosis.
Digital subtraction angiography ultimately demonstrated approximately 80% stenosis at the origin of the left internal carotid artery. More importantly, contrast stagnation persisted into the venous phase.
This finding fundamentally alters the differential diagnosis.
Persistent contrast retention implies abnormal local flow dynamics.
Blood enters the region but does not exit efficiently.
Flow stagnation is one of the major prerequisites for thrombosis.
At this point, a carotid web becomes the leading diagnostic consideration.
What Is a Carotid Web?
Carotid web is an intimal variant of fibromuscular dysplasia characterized by a thin shelf-like intraluminal projection extending from the posterior wall of the carotid bulb.
Histologically, carotid webs demonstrate:
- Intimal hyperplasia
- Smooth muscle proliferation
- Fibrosis
- Myxoid degeneration
Unlike atherosclerotic plaque, the primary danger is not progressive stenosis.
The danger lies in abnormal hemodynamics.
The web creates a low-flow recirculation zone distal to the lesion.
Blood stagnates.
Thrombus forms.
Fragments embolize distally into the middle cerebral artery circulation.
This mechanism elegantly explains:
- Recurrent ipsilateral infarction
- Failure of antiplatelet therapy
- Contrast stagnation on angiography
- Lack of conventional vascular risk factors
Why Was the Diagnosis Initially Missed?
This case illustrates several important cognitive biases.
Anchoring Bias
The carotid ultrasound abnormality was initially interpreted as intima-media thickening.
Once this interpretation was accepted, alternative explanations became less likely to be considered.
Availability Bias
Most neurologists encounter atherosclerotic carotid disease daily.
Most encounter carotid web rarely.
Common diagnoses naturally come to mind before uncommon ones.
Premature Closure
After CTA identified carotid stenosis, the diagnostic process could easily have stopped.
Yet the recurrence of stroke despite treatment should have triggered reconsideration.
Hemodynamic Evidence
One of the most fascinating aspects of this report is the computational fluid dynamics analysis.
The simulations demonstrated:
- Reduced flow velocity distal to the web
- Flow recirculation zones
- Vortex formation
- Markedly reduced wall shear stress
These findings provide direct physiologic evidence that the lesion is thrombogenic.
The carotid web was not simply an anatomic curiosity.
It was an active generator of embolic risk.
Final Clinical Diagnosis
Recurrent embolic ischemic stroke caused by a symptomatic carotid web of the left internal carotid artery with superimposed thrombus formation.
Clinical Pearls
- Carotid web is an important cause of cryptogenic stroke in younger adults.
- Recurrent ipsilateral stroke despite antiplatelet therapy should raise suspicion for carotid web.
- Degree of stenosis alone does not determine embolic risk.
- DSA remains the diagnostic gold standard.
- Flow dynamics may be more important than luminal narrowing.
- Carotid endarterectomy provides definitive treatment by removing both the web and associated thrombus.
- Careful review of CTA sagittal reconstructions may reveal subtle shelf-like lesions overlooked on routine imaging.
Key findings in the article supporting this reasoning include recurrent ipsilateral infarction despite antiplatelet therapy, DSA demonstration of severe stenosis with persistent contrast stagnation, intraoperative identification of a valve-like carotid web with adherent thrombus, CFD evidence of flow stagnation and low wall shear stress, and complete freedom from recurrent stroke after carotid endarterectomy.
Review Questions
Question 1
A 49-year-old man experiences recurrent left hemispheric ischemic strokes over a 6-week interval despite dual antiplatelet therapy. CTA demonstrates only moderate stenosis at the origin of the left internal carotid artery. Which diagnosis should be most strongly suspected?
A. Intracranial atherosclerotic disease
B. Cardioembolic stroke due to occult atrial fibrillation
C. Carotid web
D. Moyamoya disease
E. Cerebral vasculitis
Answer
C. Carotid web
Explanation
Carotid web is an underrecognized cause of recurrent ischemic stroke, particularly in younger patients without conventional vascular risk factors. Unlike atherosclerotic disease, the primary mechanism is not progressive luminal narrowing but thrombus formation within a region of flow stagnation distal to the web. Embolization of thrombotic material results in recurrent ipsilateral cerebral infarction. In this case, recurrent stroke despite appropriate antiplatelet therapy was a critical clue that a persistent thrombogenic lesion was present.
Why the Other Answers Are Incorrect
- A. Intracranial atherosclerosis typically occurs in patients with vascular risk factors and would not explain the shelf-like carotid lesion.
- B. Cardioembolism often causes infarcts in multiple vascular territories rather than recurrent ipsilateral events.
- D. Moyamoya disease produces characteristic intracranial collateral networks.
- E. Vasculitis generally presents with multifocal vascular involvement and systemic findings.
Question 2
Which imaging modality remains the diagnostic gold standard for carotid web?
A. Carotid ultrasonography
B. Magnetic resonance angiography
C. Computed tomography angiography
D. Digital subtraction angiography
E. Transcranial Doppler ultrasonography
Answer
D. Digital subtraction angiography
Explanation
Although CTA is the most commonly used noninvasive imaging modality, DSA remains the gold standard because of its superior spatial and temporal resolution. Typical findings include a shelf-like filling defect and persistent contrast stagnation into the venous phase. In this case, DSA was crucial because earlier studies were interpreted as intima-media thickening or moderate stenosis.
Why the Other Answers Are Incorrect
- A. Ultrasonography is highly operator dependent and frequently misses carotid web.
- B. MRA may identify stenosis but lacks the resolution of DSA.
- C. CTA is excellent but may produce false-negative results.
- E. Transcranial Doppler evaluates intracranial flow rather than carotid wall morphology.
Question 3
What is the primary mechanism by which carotid web causes ischemic stroke?
A. Progressive arterial occlusion from plaque growth
B. Vasospasm of the internal carotid artery
C. Hypoperfusion from critical stenosis alone
D. Thrombus formation within a low-flow recirculation zone followed by artery-to-artery embolization
E. Spontaneous arterial dissection
Answer
D. Thrombus formation within a low-flow recirculation zone followed by artery-to-artery embolization
Explanation
The shelf-like morphology of a carotid web creates abnormal flow patterns characterized by turbulence, flow stagnation, recirculation zones, and low wall shear stress. These conditions promote thrombus formation. Embolization of thrombotic material into the middle cerebral artery circulation results in recurrent ischemic stroke. Computational fluid dynamics analysis in this report demonstrated precisely these abnormalities.
Why the Other Answers Are Incorrect
- A. Progressive plaque growth describes atherosclerosis rather than carotid web.
- B. Vasospasm is not the primary mechanism.
- C. Hypoperfusion alone does not explain recurrent embolic infarction.
- E. Dissection was not present radiographically or pathologically.
Question 4
Which cognitive bias most likely contributed to delayed recognition of the carotid web in this patient?
A. Hindsight bias
B. Anchoring bias
C. Outcome bias
D. Framing effect
E. Blind obedience
Answer
B. Anchoring bias
Explanation
The initial ultrasonographic interpretation favored intima-media thickening. Once that explanation was accepted, clinicians became less likely to consider alternative diagnoses despite recurrent stroke. Anchoring bias occurs when a clinician fixates on an early diagnostic impression and inadequately adjusts in response to new information. This case illustrates how anchoring on common atherosclerotic disease can delay recognition of a rare but important diagnosis.
Why the Other Answers Are Incorrect
- A. Hindsight bias occurs after the diagnosis is known.
- C. Outcome bias judges decisions based on results.
- D. Framing effect involves influence from presentation of information.
- E. Blind obedience refers to uncritical acceptance of authority.
Question 5
Which treatment provides the most definitive elimination of the embolic source in symptomatic carotid web?
A. Aspirin monotherapy
B. Dual antiplatelet therapy indefinitely
C. Long-term anticoagulation
D. Carotid endarterectomy
E. Observation with serial imaging
Answer
D. Carotid endarterectomy
Explanation
Carotid endarterectomy directly removes the carotid web, associated thrombus, and any coexisting atherosclerotic plaque. Unlike medical therapy, which attempts to reduce thrombus formation, surgery eliminates the underlying anatomic substrate responsible for abnormal flow dynamics. In this patient, CEA resulted in restoration of vessel patency and no recurrent stroke during one year of follow-up.
Why the Other Answers Are Incorrect
- A and B may reduce thrombotic risk but do not eliminate the web.
- C has not been established as definitive therapy.
- E leaves the thrombogenic lesion untreated.
Clinical Take-Home Message
When recurrent ischemic stroke occurs in a younger patient without conventional vascular risk factors, clinicians should actively search for uncommon vascular etiologies. Carotid web is one of the most important and most frequently overlooked causes of recurrent embolic stroke. The diagnosis depends on careful review of vascular imaging, appreciation of abnormal flow dynamics, and avoidance of cognitive biases that favor more common explanations. Symptomatic carotid web should be considered a surgically remediable cause of recurrent stroke, and carotid endarterectomy can provide definitive elimination of the embolic source.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in