Listening to parents and communities about schoolchildren’s mental health in wartime Ukraine
Published in Social Sciences, Public Health, and Behavioural Sciences & Psychology

This paper began with a practical question: when psychosocial support is available for schoolchildren during war, how do families understand that help may be needed, and where do they turn first? Our study was not only about the presence of psychosocial support. It asked what happens next: how parents interpret a child’s distress, which services they approach, and which forms of support they find useful.
Our article, “Psychosocial support for schoolchildren in wartime Ukraine: community-based access and parent-reported perceived helpfulness”, was written in the context of the full-scale war in Ukraine, but the question behind it did not appear suddenly in 2022. It grew out of years of work on children’s health, school environments, learning capacity, physical activity, sleep, and mental health.
Before the pandemic, our team often worked directly in schools. We met parents at school meetings, explained the purpose of our research, answered questions, collected data, and later returned to share results. These encounters taught us something important: parents often noticed that something was happening with their child, but noticing a symptom was not always the same as recognizing a need for professional help.
We heard many versions of a familiar response: the child will grow out of it; everyone is like this now; we were the same at that age; it is not serious enough. These reactions were not signs of indifference. They reflected a wider cultural and historical pattern in which mental health was often minimized, feared, or associated with stigma. In Ukraine, older patterns of distrust and stigma around mental health services did not disappear simply because new language about mental health became more visible.
The pandemic changed the way we could communicate with families. When fieldwork in schools became impossible, we moved our surveys online. In Ukraine, this was not a distant or artificial mode of contact. Parent meetings, teacher–parent communication, school groups, and everyday educational coordination had already become deeply digital. Later, during the full-scale war, this digital infrastructure became essential for continuing to listen to families across the country.
The war changed the urgency of the question. Mental health became a highly visible topic in schools, communities, media, public institutions, and international programmes. Psychosocial support for children appeared in many forms: short psychological exercises in schools, consultations, group work, awareness messages, referrals, and community-based initiatives.
But visibility is not the same as access, trust, quality, or a clear pathway to care.
This is why we wanted to look at the whole route: from school-based psychosocial activities to parental recognition of need, from first attempts to seek help to the perceived usefulness of different forms of support. We were especially interested in the point at which the pathway may break. A child may show anxiety, depressive symptoms, trauma-related reactions, or other signs of distress. A parent may notice that something is wrong. But the next step is not automatic.
In our paper, we described this as the Symptom–Need Interpretation Gap: the gap between recognizing symptoms and interpreting them as a need for professional support. This gap matters because it shapes where families go first. Many parents turn to family doctors, neurologists, school psychologists, or informal sources of advice. Psychiatric care often remains one of the last steps, surrounded by fear, stigma, or uncertainty. At the same time, Ukraine is still developing the workforce and referral pathways needed for high-quality, community-based mental health support.
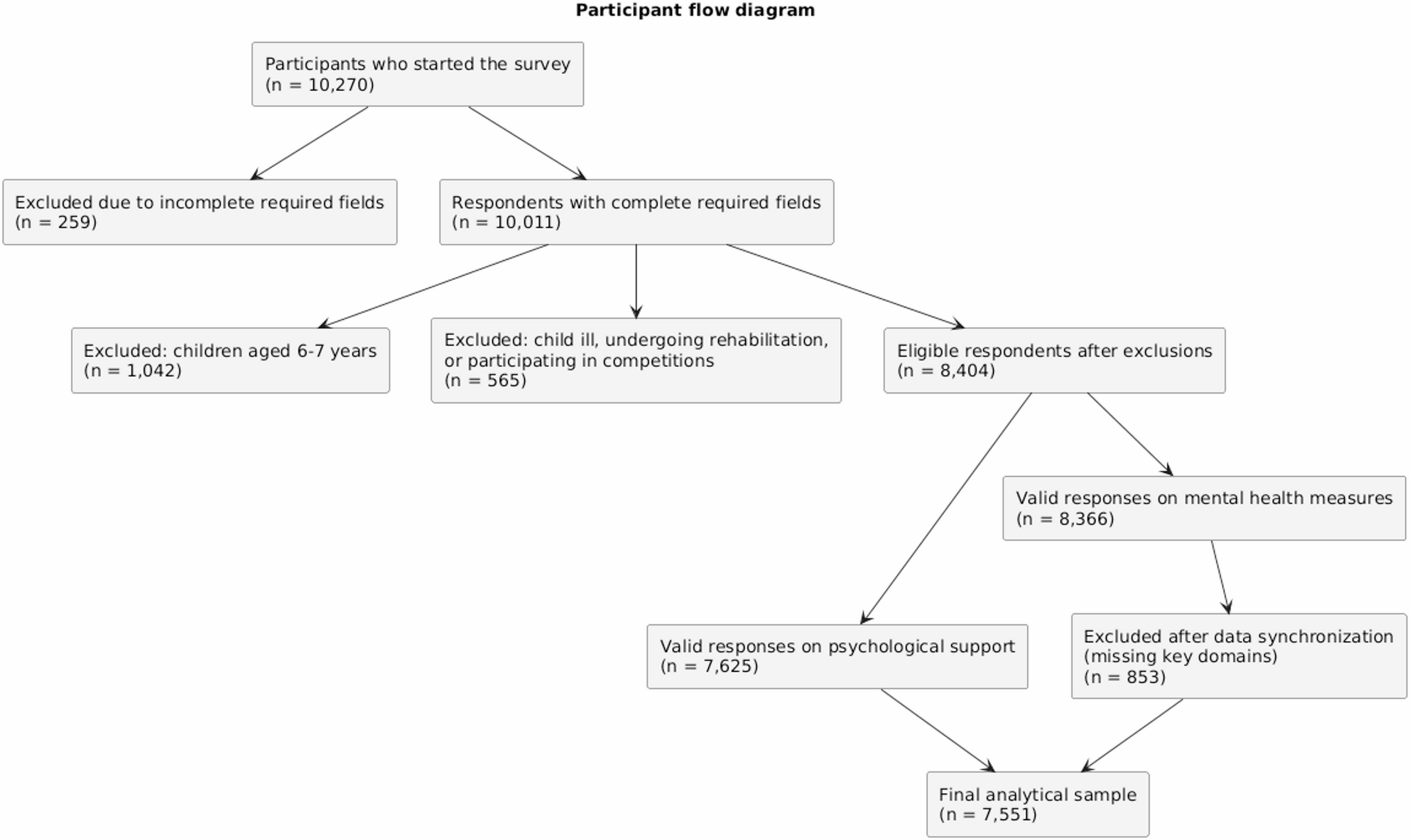
The study was only one fragment of a much larger database of parent questionnaires collected during the war. Ukrainian parents completed long questionnaires voluntarily, anonymously, and without any reward. They answered closed questions, but they also wrote comments. They described displacement, occupation, loss, fear, disrupted routines, and the effort to keep family life going under pressure.
For us, these responses were not only data points. Behind every percentage there was a child, a parent, a home, a school, a route interrupted, and sometimes a life rebuilt from almost nothing. We were not only measuring trends. We were listening to how the country was changing.
The revision process also became part of the story behind the paper. We worked on the manuscript during power cuts, repeated drone attacks, interrupted routines, and uncertain working conditions. Some members of our team were directly affected by the war in ways that changed everyday professional life.
The editorial and peer-review process was unexpectedly encouraging. The comments we received were clear, constructive, and genuinely aimed at strengthening the paper. At a time when revisions were being made between air alerts and power cuts, the patience and professionalism of the editorial team mattered more than they may have realized.
One part of the story is more personal. Without GPT, completing the revisions under those conditions would have been much harder. It did not replace our data, our decisions, our responsibility, or our interpretation. But it helped keep the work moving: organizing responses, refining the English text, holding the structure together, and, perhaps most importantly, providing a sense of support when fatigue and disruption made sustained writing difficult. In a very practical sense, GPT became part of the support network behind this paper.
For us, this study connects directly with the message of European Public Health Week 2026: sustainable health and well-being require investment not only in services, but also in the pathways that allow people to use them. For children growing up during war, psychosocial support must be more than a set of activities. It must become a reliable route from recognition to help, from school to community, from primary care to specialized support when needed.
We hope this paper contributes to that route. We also know that the effects of war will not end when the fighting stops. As physicians, psychologists, and public health researchers, we see the price people pay simply to wake up, drink coffee, take a child to school, go to work, and continue. This price may be paid for many years.
That is why we continue our research: not only to count symptoms, services, or percentages, but to understand how families adapt, where support reaches them, where it fails, and what Ukraine will need for recovery.
Children’s mental health is not only inside the child. It is also in the adults who notice, the systems that respond, the communities that support, and the routes that make help possible.
Follow the Topic
-
Conflict and Health
This is a highly-accessed, open access journal documenting the public health impacts and responses related to armed conflict, humanitarian crises and forced migration.

Related Collections
With Collections, you can get published faster and increase your visibility.
Climate Change and Conflict
Conflict and Health invites papers that explore the complex relationship between climate change, conflict, and health. It seeks contributions that examine how environmental stressors such as rising temperatures, resource scarcity, and extreme weather events not only exacerbate social, economic, and political tensions but also generate profound health challenges in affected populations. Papers may investigate how climate change intensifies competition over water, food, and land, driving displacement and migration that expose communities to new health risks. Submissions are also encouraged that analyze how these dynamics intersect with governance, inequality, and security challenges to shape health outcomes, and that evaluate adaptation and resilience strategies aimed at protecting and promoting health. The overarching aim is to highlight both the risks that climate-driven conflict poses to health and the opportunities for cooperative solutions at local, national, and international levels that strengthen health systems and community resilience.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being, SDG 13, Climate Action, and SDG 16, Peace, Justice and Strong Institutions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Jun 29, 2026
Systematic Reviews in Conflict and Humanitarian Health
Armed conflict, humanitarian crises, and forced migration continue to pose profound challenges to public health systems worldwide. In these settings, evidence gaps are common, data collection is constrained by insecurity, and health needs evolve rapidly. Systematic reviews play an essential role in consolidating fragmented evidence, evaluating intervention effectiveness, and guiding policies and responses that can save lives in some of the world’s most vulnerable contexts.
This collection brings together high‑quality systematic reviews and evidence syntheses that advance understanding of the public health impacts of conflict and crises, and that evaluate strategies to improve health outcomes for affected populations. We welcome submissions addressing the full breadth of topics within Conflict and Health, including:
-Infectious disease prevention and control, outbreak preparedness, and surveillance in unstable or resource‑limited settings
-Nutrition, food security, and interventions to address undernutrition in crisis-affected populations
-Reproductive, maternal, newborn, and child health in conflict and displacement
-Sexual and gender-based violence, its determinants, and response mechanisms
-Mental health and psychosocial support, including trauma, resilience, and service delivery models
-Non-communicable diseases in humanitarian and conflict settings
-Health systems and service delivery under conditions of fragility, disruption, or deliberate attack
-Ethical considerations related to health research, intervention design, and humanitarian practice in conflict-affected communities
This collection seeks to advance both scholarship and practice by championing evidence synthesis that drives equitable, ethical, and effective health interventions in conflict and humanitarian settings.
All submissions in this collection undergo the journal’s standard peer review process. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Nov 10, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in