Repurposing a Simplified Diagnostic Tool to Increase Screening for HBV and HCV in Resource-limited Settings
Published in Public Health

Hepatitis B (HBV) and C (HCV) infections are a public health threat, affecting an estimated 254 million and 50 million people, respectively. Particularly, in sub-Saharan Africa (sSA), HBV is widespread, and HCV is no exception. It too poses a significant problem for the African population. According to figures provided by the World Health Organization (WHO), about 6% of sSA communities are HBsAg positive, whilst HCV prevalence ranges from 1% to 2%.
But, what if we could use already existing tools or approaches in other diseases to help reduce the current burden of viral hepatitis? In today’s blog post, we dive into the motivations and trademark features of a novel study that took place in both Uganda and Cameroon between May 2021 and March 2023, and what it could mean for those undiagnosed with either HBV or HCV. Read more below!
What inspired this study?
We started this study because the PI was intrigued by the plasma separation card (PSC), which he saw presented at a conference, and its potential applications. At that time it was not in use in the field for viral hepatitis, only having been recently validated in a laboratory in Barcelona.
Its capability to collect dried blood samples to monitor HIV viral loads got us thinking that, perhaps, this could work for other diseases and in resource-limited areas like Cameroon and Uganda, where it is not easy to perform phlebotomies (drawing blood). However, not only could the PSC be transported and store samples without the need to be maintained in cold chain, but it would not require further centrifugation plasma separation. Also, sampling could be carried out via whole capillary blood obtained by fingerstick.
This then led us to carry out a real-world study and examine the feasibility and acceptability of the PSC in viral hepatitis testing. With context-adapted and simplified screening methods, screenings overall could rise and possibly result in a higher number of timely diagnoses.
In the case of viral hepatitis infections, this was extremely important to us. Although the World Health Organization (WHO) set elimination targets, timely screening and diagnosis for viral hepatitis remains the main obstacle in reaching these objectives.
Why is this study important?
Countries with mid- and high prevalence of viral hepatitis infections often find themselves with scarce resources for healthcare. This results in a substantial hurdle for establishing accessible screening opportunities. Both late diagnosis of viral infection and their subsequent late access to adequate care mean that those with either HBV or HCV can face life-threatening conditions–all of which are preventable.
Our desire to explore feasible and affordable diagnostic tools would not only represent a step towards promoting equitable access and screening services, but it would also entail improving health outcomes overall.
But, there is more. We wanted to maximise the potential impact and implementation of these diagnostic tools, so we also explored patients’ perspectives, experiences and preferences.
What makes this study unique?
This study was unique because it recognised that introducing a new point-of-care test would be meaningless if patients themselves were reluctant to accept such an approach.
Our study further contributed to closing the existing gap in current research and literature in SSA.
Did this study show anything unexpected?
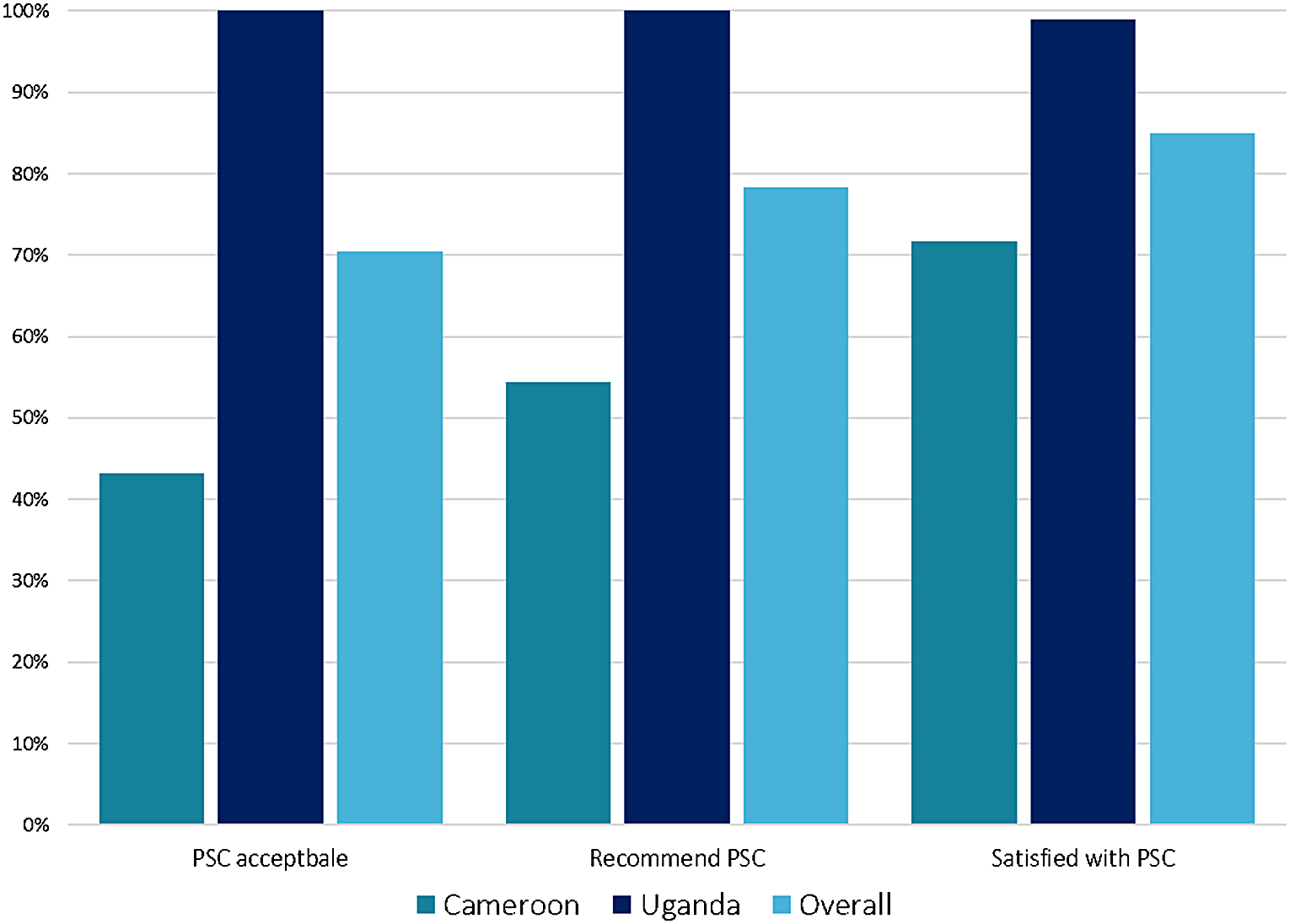
Although not unexpected per se, we did find that there were major differences between the countries on acceptability of the PSC method (100% in Uganda vs 43% in Cameroon). This suggests that once again, there is no one-size-fits-all.
“The PSC method could be feasible for viral hepatitis testing, but acceptability thereof is not always guaranteed. Exploring these variations, like in the case of Cameroon and Uganda, implies enhancing care according to the person, and not just to the infection.”
What is the wider significance of the study’s findings?
One take-away is that we can develop and integrate simplified diagnostic tools effectively in resource-limited settings.
Secondly, by exploring insights from clients (aka patients), we can form strategies that better match the needs of different communities and help make sure that interventions both work and are well-received.
Finally, it’s worth mentioning that this study is another contributing piece to our research team’s extensive work on understanding and implementing simplified diagnostic tools for viral hepatitis infection screenings. For example, as part of a EU-funded project “Viral Hepatitis COMmunity Screening, Vaccination, and Care (VH-COMSAVAC)”, we were able to screen around 1,000 migrants in Catalonia, Spain, using PSCs–alongside rapid diagnostic tests (RDTs)–to examine HBV viral load and hepatitis D virus (HDV) antibodies, and identify past-resolved HBV infections.
Overall, there is much more to explore with the use of PSCs in resource-limited settings, like that of HIV clinics in Uganda and Cameroon, and in community-based settings in Spain as well. More related work can be found below:
- Picchio CA, Kwakye DN, Rando-Segura A, et al., Lazarus JV. Community-based screening enhances hepatitis B virus (HBV) linkage to care among West African migrants in Spain. Communications Medicine 2023.
- Picchio CA, Kwakye DN, Gómez Araujo S, et al., Lazarus JV. A novel model of care for simplified testing of HBV in African communities during the COVID-19 pandemic in Spain. Scientific Reports. 2021.
- Lazarus JV, Herranz A, Picchio CA, et al. Eliminating hepatitis C on the Balearic Islands, Spain: a protocol for an intervention study to test and link people who use drugs to treatment and care. BMJ Open. 2021.
- MacKinnon MJ, Picchio CA, Kwakye DN, et al., Lazarus JV. Chronic conditions and multimorbidity among West African migrants in greater Barcelona, Spain. Frontiers Public Health. 2023.
Follow the Topic
-
Journal of Epidemiology and Global Health
The journal aims to impact global epidemiology and international health with articles focused on innovative scholarship and strategies to advance global health policy.

Related Collections
With Collections, you can get published faster and increase your visibility.
Climate and Environmental Change as Drivers of Infectious Disease: A Planetary Health Perspective
Human health is increasingly shaped by the interconnected pressures of climate change, environmental degradation, and socio‑ecological disruption. These planetary‑scale changes influence not only the epidemiology of infectious diseases, but also the public health systems, social structures, and community capacities that determine exposure, vulnerability, and resilience. This Collection adopts a planetary health perspective to explore how climate variability, ecosystem disruption, and human–environment interactions affect infectious disease risks and the public health responses needed to address them.
We welcome research that examines how shifts in temperature, precipitation, humidity, extreme weather events, land‑use change, biodiversity loss, and urbanization influence pathogen ecology, transmission pathways, and population vulnerability. Beyond epidemiological patterns, the Collection seeks contributions that address preparedness, surveillance, health system resilience, risk communication, governance, and cross‑sectoral interventions aimed at mitigating and adapting to climate‑related infectious disease threats.
Studies leveraging epidemiological datasets, climate and environmental records, spatial mapping, and predictive modeling are encouraged, as are qualitative, policy‑focused, and implementation‑oriented works that illuminate barriers and opportunities within public health systems. Particular attention is given to inequities in exposure and resilience, the needs of high‑risk populations, and the role of community‑level and institutional adaptation strategies.
By integrating epidemiology, environmental science, and public health practice, this Collection aims to advance understanding of climate–disease interactions, strengthen early warning and response systems, and inform adaptive strategies that protect and promote planetary health in a rapidly changing world. Topics of interest include but are not limited to:
- Climate‑sensitive infectious diseases and changing transmission patterns
- Impacts of extreme weather events and environmental disruption on disease risk
- Public health preparedness, surveillance, and early warning systems
- Health system resilience and climate adaptation strategies
- Socio‑ecological vulnerability, inequities, and community resilience
- Land‑use change, biodiversity loss, and zoonotic spillover
- Modeling climate, environmental, and disease interactions
- Governance, policy, and multisectoral responses to planetary health threats
- One Health and Planetary Health approaches to infectious disease prevention
This Collection supports and amplifies research related to SDG 13, Climate actions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 31, 2027
Public Health Professionals’ Education
Strengthening the education and continuous professional development of public health professionals is fundamental to achieving resilient, equitable, and responsive health systems. Recent global experiences including pandemics, protracted humanitarian crises, climate-related health risks, rapid urbanization, and technological transformation have highlighted both the critical role of the public health workforce and persistent gaps in training relevance, scale, quality, and sustainability. In many settings, educational models remain insufficiently aligned with real-world system needs, emerging competencies, and evolving career pathways.
While there is growing innovation in public health education, evidence and lessons learned are dispersed across disciplines and regions. A focused supplement in the Journal of Epidemiology and Global Health will provide a timely scholarly platform to consolidate high-quality research and practice-based insights.
The proposed Collection aims to advance knowledge in the education of public health professionals by:
Showcasing empirical evidence and innovative models for public health education and training
Examining how educational approaches align with health system priorities and workforce needs
Informing policy, institutional strategies, and investment in public health workforce development
Promoting equity, quality, and sustainability in public health education globally.
Scope and Thematic Areas
The supplement will invite original research articles, systematic or scoping reviews, and rigorously documented practice-based papers across the following thematic areas:
Competency-Based Public Health Education
- Core and advanced competency frameworks
- Alignment of curricula with population health needs and system priorities
Field-Based and Applied Learning Models
- Field Epidemiology Training Programs (FETPs) and similar applied training models
- Experiential learning, service-based education, and community engagement
Interprofessional and Multisectoral Education
- Collaborative training across health, social, environmental, and humanitarian sectors
- Preparing public health professionals for whole-of-government and whole-of-society approaches
Digital, Blended, and Distance Learning Innovations
- Online and hybrid training models
- Use of digital platforms, simulation, and emerging technologies in education
Education for Health Emergencies and Fragile Settings
- Workforce training for outbreak preparedness, humanitarian response, and conflict settings
- Adaptive education models in fragile and resource-constrained contexts
Equity, Ethics, and Inclusion in Public Health Training
- Gender, geographic, and socioeconomic equity in access to education
- Ethical dimensions of training, mentorship, and professional advancement
Leadership, Management, and Systems Thinking
- Training for public health leadership, governance, and policy engagement
- Building managerial and strategic competencies for system-level impact
Mentorship, Supervision, and Career Pathways
- Structured mentorship and supervision models
- Transition from training to practice and career progression
Monitoring, Evaluation, and Impact of Public Health Education
- Methods for assessing educational outcomes and workforce impact
- Long-term sustainability and return on investment of training programs
Partnerships, Financing, and Institutionalization
- Academic–government–partner collaborations
- Financing models and institutional integration of training programs
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Dec 17, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in