SSRI-Induced Bruxism: Recognizing an Underappreciated Adverse Effect in Clinical Practice
Published in Neuroscience and Biomedical Research
Selective serotonin reuptake inhibitors (SSRIs) are widely prescribed and generally well tolerated; however, movement disorders associated with serotonergic agents remain underrecognized. A recent case in the Journal of Medical Case Reports highlights SSRI-induced bruxism as an important and potentially reversible adverse effect with clear clinical implications.
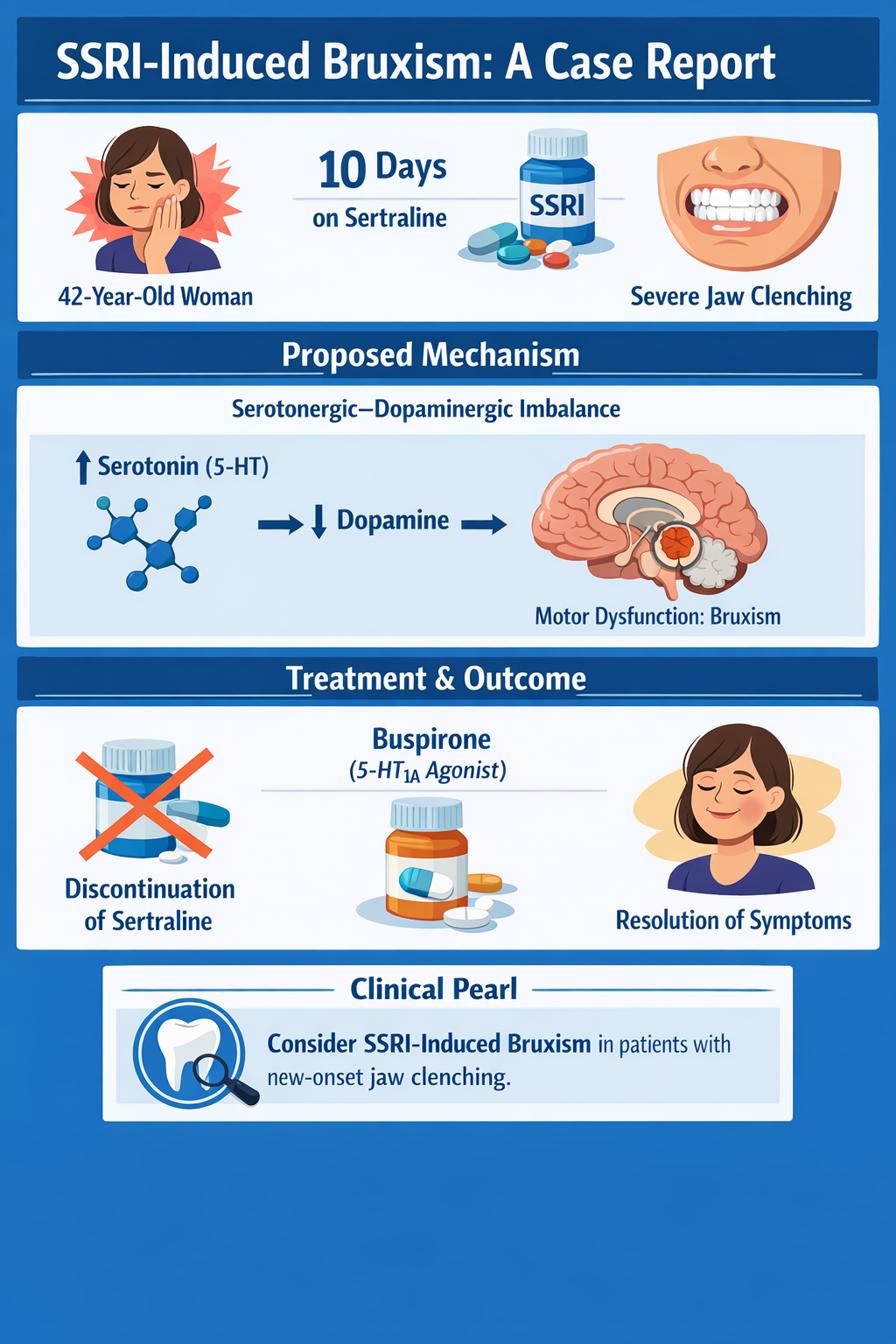
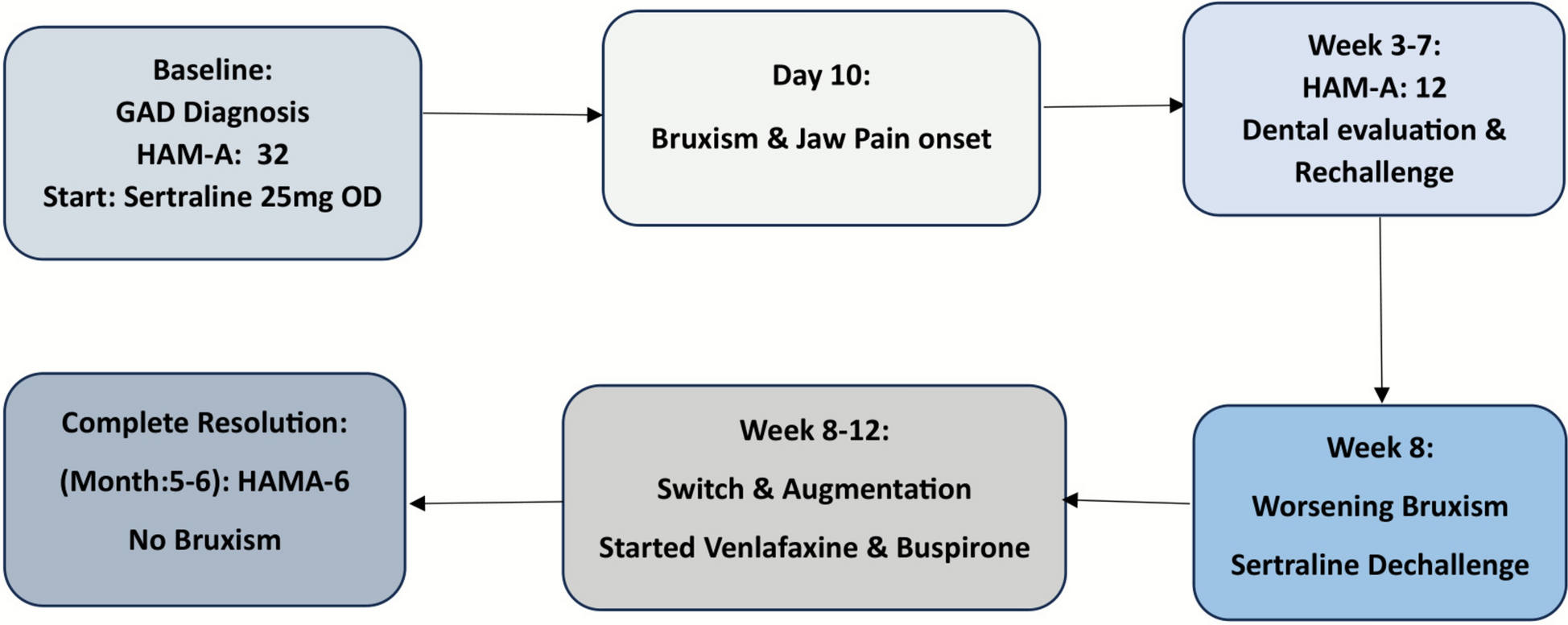
In this report, a 42-year-old woman developed severe, persistent daytime jaw clenching approximately 10 days after initiating sertraline therapy. She had no prior history of bruxism, temporomandibular joint dysfunction, or other movement disorders. The temporal relationship between medication initiation and symptom onset was notable. Despite dose adjustment, her symptoms persisted, raising concern for a medication-induced etiology. Following discontinuation of sertraline, her bruxism resolved, supporting causality. Additional symptomatic improvement was achieved with initiation of buspirone.
The underlying pathophysiology is thought to involve serotonergic–dopaminergic imbalance. Increased synaptic serotonin from SSRI use can inhibit dopaminergic activity within central motor pathways, particularly in basal ganglia circuits. This relative dopaminergic suppression may manifest clinically as extrapyramidal-type symptoms, including bruxism. Buspirone, a 5-HT1A partial agonist, is believed to exert therapeutic benefit by modulating serotonergic tone and indirectly restoring dopaminergic activity, thereby alleviating abnormal motor activity.
This case underscores several key clinical lessons. First, clinicians should maintain a high index of suspicion for medication-induced movement disorders when new-onset motor symptoms follow SSRI initiation. Second, careful medication review may obviate the need for extensive dental, neurologic, or imaging evaluations. Third, management strategies may include dose reduction, discontinuation, or pharmacologic augmentation (e.g., buspirone) depending on clinical context and psychiatric necessity.
Importantly, this case contributes to the growing body of literature emphasizing the role of case reports in identifying uncommon adverse drug reactions and refining clinical practice. Early recognition and appropriate management can significantly improve patient outcomes while avoiding unnecessary interventions.
Question:
Which pharmacologic approach is most appropriate for treating SSRI-induced bruxism?
A) Dopamine antagonism with haloperidol
B) Beta-adrenergic blockade with propranolol
C) Serotonin 5-HT1A partial agonism with buspirone
D) Benzodiazepine sedation with clonazepam
Answer:
C) Serotonin 5-HT1A partial agonism with buspirone
Mechanism: Buspirone acts as a partial agonist at presynaptic and postsynaptic 5-HT1A receptors, reducing excessive serotonergic activity and facilitating restoration of dopaminergic tone within central motor pathways. This helps reverse SSRI-induced suppression of dopamine and alleviates bruxism.
Clinical Pearl / Take-Home Message:
New-onset bruxism shortly after initiating an SSRI should prompt consideration of a medication-induced movement disorder; early recognition and treatment—often with dose adjustment, discontinuation, or addition of buspirone—can rapidly resolve symptoms and prevent unnecessary diagnostic workup.
Read the full case:
https://jmedicalcasereports.biomedcentral.com/articles/10.1186/s13256-026-05834-1
Explore more from JMCR:
https://jmedicalcasereports.biomedcentral.com/
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in