Understanding “Colon Age”: A New Approach to Colorectal Cancer Screening
Published in Biomedical Research


Because of the growing trend in early-onset colorectal cancer (CRC) among younger populations (1), the U.S. Preventive Services Task Force recently shifted their recommendation from starting CRC screening at age 50 to age 45. There remains a catch: even if uptake of these screening recommendations is high among 45-49 year olds, half of early-onset CRC cases will be missed prior to development of signs and symptoms. It is estimated that around 30-35% of the eligible U.S. population 45-75 years old is not current with screening (2). With the long-term goal of determining who should be considered for early screening, we sought to contribute to improving prevention and early detection of early-onset CRC.
A Closer Look at a High-Risk Group
CRC is the most common cause of visceral cancer death in men younger than age 50 (1). Male veterans, in particular, may be at higher risk for CRC than non-veterans due to differences in lifestyle factors and perhaps certain environmental exposures. To identify specific risk factors for early-onset CRC in this population, we acquired and examined data from the electronic medical records of 600 male Veterans with CRC aged 35 to 49 and compared them to two matched control groups—one based on colonoscopy findings and the other from general clinic visits (3).
We analyzed these data using a split-sample approach: a derivation dataset (used to develop the model) and a validation dataset (used to test it). Following full model analysis, we developed two models – one model with 15 key risk factors, and a simpler one with 7. Both performed well in identifying risk for early-onset CRC. Some “standout” risk factors included: no service-connected disability, higher comorbidity index, family history of CRC, and not using NSAIDs or statins.
Making Risk Relatable
A challenge in clinical and preventive medicine is how to relate risk factors to “risk” for an individual patient. This concept is important for considering not only whom to screen early, but also how. People often relate how “old” they feel or how their body functions relative to their age; we applied this paradigm to CRC screening. We applied our validated 15- and 7-variable models to create a new measure for understanding an individual’s risk for CRC and, by extension, their personalized need for CRC screening (4).
We refer to this metric as “Colon Age”, which indicates the biological age of a person’s colon by combining their individual risk profile with population-based CRC occurrence rates. This is achieved by multiplying a patient’s specific risk factors (as identified in the 15- or 7-variable model) with their Surveillance, Epidemiology and End Results (SEER) age-specific rate. Think of being told, “you have the colon age of a 60-year-old” to someone who is only 45 years old.
What Do Patients and Providers Think?
Colon Age is intended to express a patient’s individual risk for CRC in terms that are relatable. Given the absence of evidence for superiority of any single screening strategy, often primary care providers are relied upon to bring up screening during annual exams. Therefore, we completed two qualitative studies regarding the perceived clinical utility and acceptance of simple CRC risk prediction tools.
Round 1: In interviews with 15 patients and 15 primary care providers, we asked about the facilitators and barriers of a simple five-variable risk prediction model in clinical practice (5). Providers had concerns regarding the tool’s accuracy and consistency with guidelines, but both patients and providers agreed that such a tool would generate discussion about CRC screening in clinic and potentially increase screening uptake.
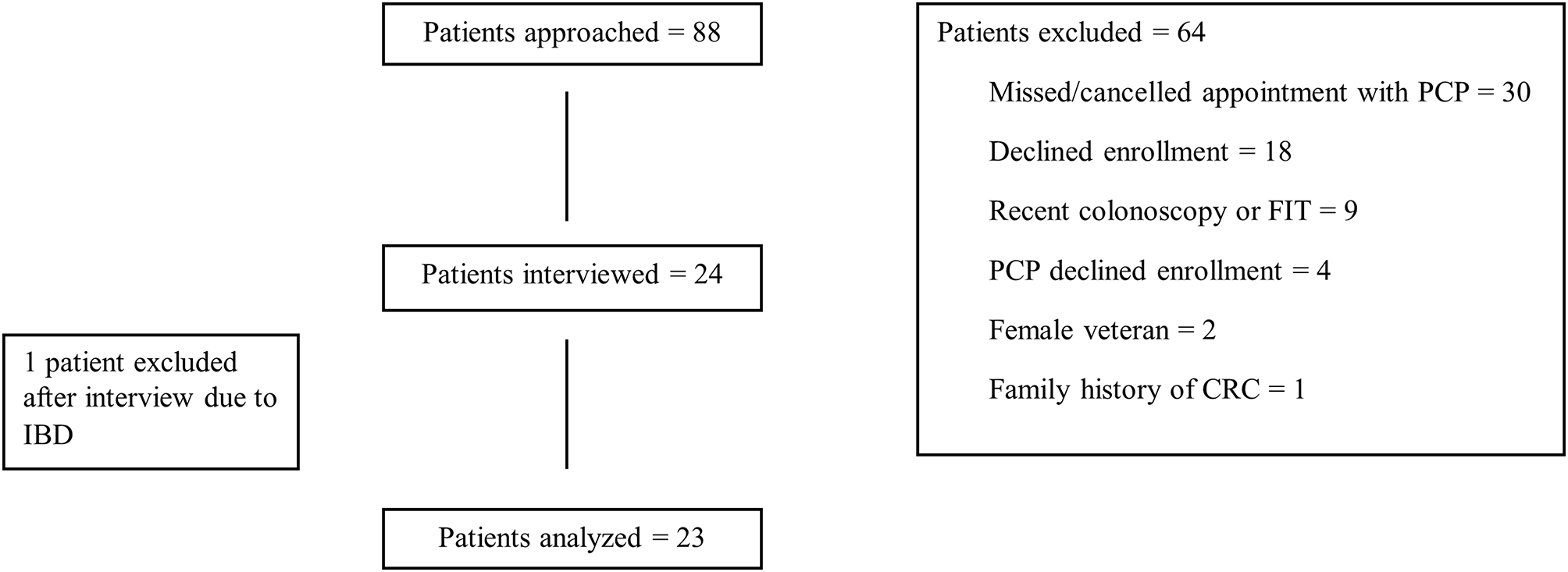
Round 2: We received similar feedback when interviewing 24 patients and 8 primary care providers using the validated 7-variable Colon Age model (6). Patients found the tool easy to understand, as well as empowering in terms of being informed and making their own decisions about CRC screening. Providers agreed that the Colon Age metric may allow greater patient autonomy regarding CRC screening at a time when patients are hesitant to get screened prior to age 50. The Colon Age tool was perceived as a way to get patients involved in their screening decisions, and 96% of the patients we interviewed agreed to have their Colon Age calculated.
There remain some concerns. Time is tight during clinic visits. Some patients were hesitant to share too much personal information, and both groups just wanted to know more about how the tool actually works. Some providers likened the Colon Age tool to the increasingly important concept of precision medicine.
Moving Forward: Precision, Personalization, and Prevention
Despite some limitations, the Colon Age tool appeared to be acceptable and useful to patients and providers in individualizing risk for CRC. It certainly isn’t a silver bullet, but the metric may be a helpful tool for getting high-risk people 45-49 years old screened for CRC (as is currently guideline-recommended) and those younger than age 45 screened sooner, if thought to be clinically appropriate. Colon Age also reflects the growing push toward precision medicine and shared decision-making, two trends that are shaping the future of primary care.
By allowing patients and providers to talk more openly and accurately about individual risk, they can work toward making informed, personalized decisions on when and how to get screened—because catching CRC early can save lives.
References:
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024 Jan;74(1):12–49.
- Lin JS, Piper MA, Perdue LA, et al. Screening for colorectal cancer: updated evidence report and systematic review for the US preventive services taskforce. JAMA. 2016;315(23):2576–94.
- Imperiale TF, Myers LJ, Barker BC, et al. Risk Factors for Early-onset Sporadic Colorectal Cancer in Male Veterans. Cancer Prev Res. 2023;16(9):513–522.
- Imperiale TF, Myers LJ, Barker BC, et al. Colon Age: A Metric for Whether and How to Screen Male Veterans for Early-Onset Colorectal Cancer. Cancer Prev Res. 2024;17(8):377–384.
- Matthias MS & Imperiale TF. A risk prediction tool for colorectal cancer screening: a qualitative study of patient and provider facilitators and barriers. BMC Fam Pract. 2020;21, 43.
- Imperiale TF, Cheng M, Thomas MR et al. A qualitative study of a new metric for estimating early-onset colorectal cancer risk in male veterans: “Colon Age”. BMC Prim. 2025;26, 226.
Follow the Topic
-
BMC Primary Care
Previously known as BMC Family Practice, this is an open access, peer-reviewed journal that considers articles on all aspects of primary health care research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Sleep health and primary care
Sleep health is a critical yet often overlooked aspect of overall well-being, particularly in the context of primary care. Sleep disorders, including insomnia and obstructive sleep apnea, can significantly impact patients' physical and mental health, leading to complications that may complicate primary care management. Sleep issues are becoming increasingly recognized for their chronicity, widespread prevalence, and influence on other chronic conditions. Therefore, understanding the relationship between sleep health and primary care practices is vital. This Collection aims to explore the intersection of sleep health and primary care, shedding light on innovative approaches to assessment and treatment.
Continued exploration in this area could pave the way for groundbreaking advancements in the management of sleep health care within primary care settings. As more research is conducted, we may see innovative approaches to screening and treating sleep disorders that can assist primary care providers in addressing these issues more effectively and efficiently. Future studies may also illuminate the impact of sleep health on chronic disease prevention and management, ultimately leading to a more holistic approach to patient care. By enhancing sleep health awareness among primary care providers, we can promote comprehensive care that acknowledges the crucial role of sleep.
We invite submissions on a range of topics that include, but are not limited to:
- Management of insomnia in primary care
- Management of obstructive sleep apnea in primary care
- The intersection between sleep disturbances and chronic disease
- Integrated behavioral health approaches to the management of sleep disorders
- Screening tools for sleep disorders in primary care
- Implementation of new models of care for sleep disorders
This Collection supports and amplifies research related to SDG 3: Good Health and Well-being.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 07, 2027
Managing substance use disorders
Substance use disorders are a multifaceted issue that poses significant challenges to primary care providers and the healthcare system at large. This Collection aims to explore various dimensions of substance use management, including the identification and treatment of drug, alcohol, and tobacco use disorders. Research that focuses on screening, diagnosis, and risk assessment in primary care settings is particularly valuable in understanding how to effectively manage these disorders and reduce their impact on individuals and communities.
Understanding and addressing substance use disorders is crucial for enhancing public health outcomes and ensuring the well-being of patients. Recent advances in screening tools and interventions have shown promise in identifying individuals at risk and providing them with appropriate support and treatment. By fostering collaboration between primary care providers, mental health professionals, and community organizations, we may witness a significant shift in how substance use is perceived and managed, ultimately improving health outcomes and quality of life for affected individuals.
We invite submissions on a range of topics that include but are not limited to:
- Innovative screening methods for substance use disorders
- Interventions for alcohol use disorders
- Management strategies for tobacco cessation
- Risk assessment approaches in primary care
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Sep 08, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in