When SIADH Meets PRES: A Rare Neuroendocrine Link Uncovered
Published in Neuroscience and Biomedical Research
Explore the Research
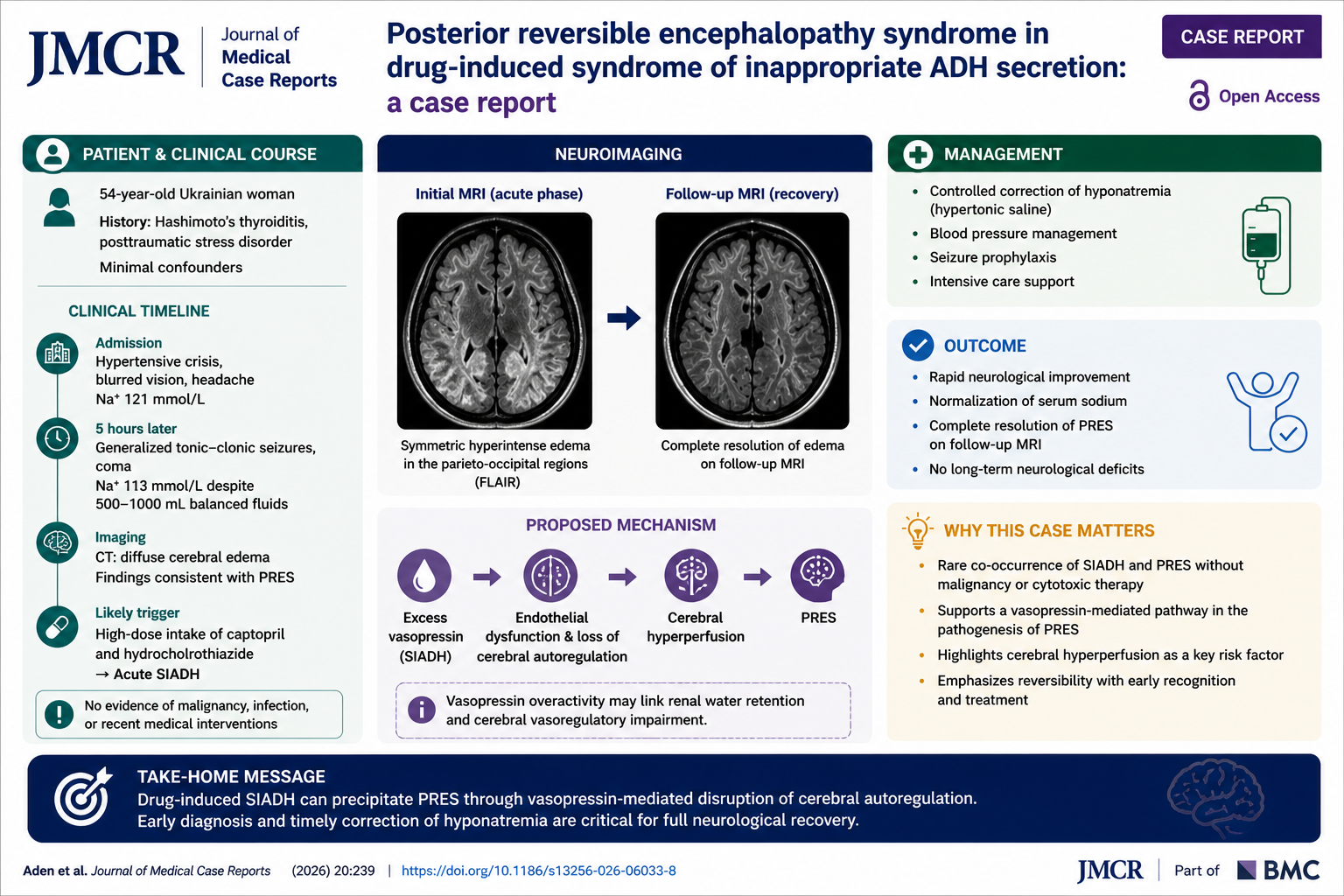
Posterior reversible encephalopathy syndrome in drug-induced syndrome of inappropriate ADH secretion: a case report
Case summary
In this case report from the Journal of Medical Case Reports, Aden and colleagues describe a 54-year-old woman who developed acute drug-induced SIADH followed by PRES.
The patient presented with hypertensive crisis, headache, and visual disturbances. Initial labs showed hyponatremia (Na⁺ 121 mmol/L), which rapidly worsened to 113 mmol/L within hours. This deterioration coincided with high-dose ingestion of captopril and hydrochlorothiazide—likely triggering SIADH.
Her clinical course escalated dramatically:
Generalized tonic–clonic seizures
Coma
Diffuse cerebral edema on CT imaging
Neurologic evaluation confirmed PRES, supported by visual symptoms, hypertension, and characteristic imaging findings.
Despite severe presentation, the patient improved with:
Controlled correction of hyponatremia using hypertonic saline
Blood pressure management
Supportive intensive care
Remarkably, she made a full neurological recovery within days, and follow-up MRI showed complete resolution of PRES, with no long-term deficits.
Why this case matters
This report is notable for several reasons:
Uncommon association: SIADH and PRES are rarely reported together in otherwise healthy individuals without malignancy or chemotherapy.
Mechanistic insight: The case supports a shared pathway involving vasopressin (AVP) overactivation, potentially affecting both renal water handling and cerebral vascular regulation.
Cerebral autoregulation: Findings reinforce the role of cerebral hyperperfusion and endothelial dysfunction in PRES pathogenesis.
Reversibility: Timely recognition and correction of the underlying trigger can lead to complete neurological recovery, even after severe presentation.
Clinical take-home message
Acute, drug-induced SIADH can precipitate PRES through vasopressin-mediated dysregulation of cerebral perfusion. Early recognition and prompt correction of hyponatremia are critical to achieving full neurological recovery.
Question:
Which mechanism most plausibly links SIADH to the development of PRES in this case?
A. Direct neuronal toxicity from hyponatremia
B. Autoimmune-mediated demyelination
C. Vasopressin-mediated dysregulation of cerebral blood flow
D. Primary intracranial infection
Correct answer:
C. Vasopressin-mediated dysregulation of cerebral blood flow
Explanation:
Excess vasopressin activity in SIADH may contribute to impaired cerebral autoregulation and endothelial dysfunction, promoting hyperperfusion and vasogenic edema—key features in PRES pathophysiology.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in