Asymptomatic Multisegmental Epidural Hematoma After Unilateral Biportal Endoscopic Lumbar Decompression: Challenging Conventional Surgical Paradigms
Published in Neuroscience and Biomedical Research
Explore the Research
Asymptomatic multisegmental epidural hematoma following unilateral biportal endoscopic lumbar decompression: a case report
Case summary
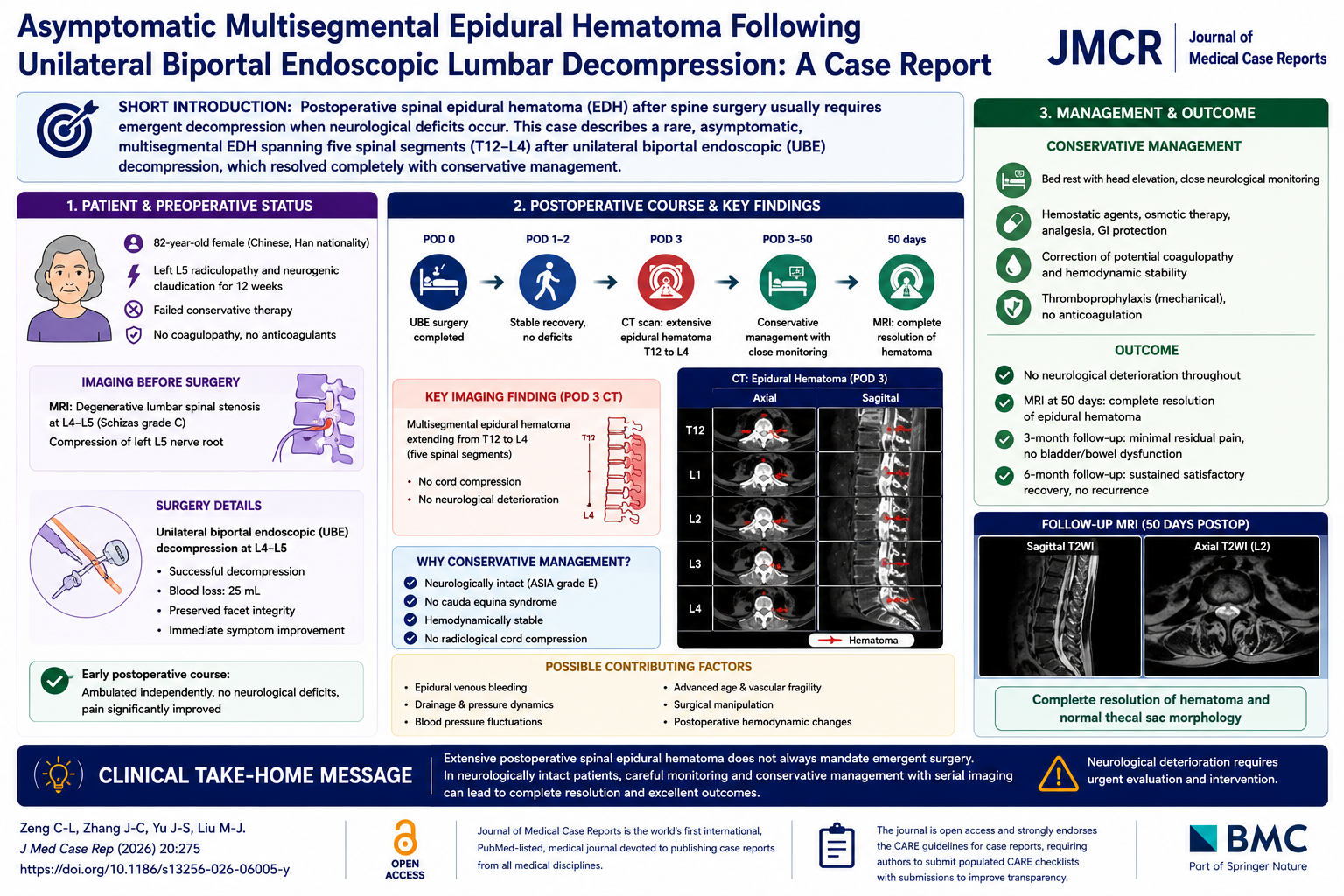
In this report, Zeng and colleagues describe an 82-year-old Chinese woman with severe left L5 radiculopathy and neurogenic claudication caused by L4–L5 degenerative lumbar spinal stenosis. Conservative therapies including physiotherapy and medication had failed, and the patient underwent unilateral biportal endoscopic (UBE) decompression.
The surgery was technically successful, with minimal blood loss (25 mL), preserved facet integrity, and immediate improvement in radicular symptoms. Early postoperative recovery was uneventful, with independent ambulation and no neurological deficits.
Unexpectedly, postoperative day 3 CT imaging demonstrated extensive multisegmental epidural hematoma extending from T12 to L4. The imaging findings on page 3 show longitudinal hematoma spread across multiple spinal levels without evidence of cord injury or progressive compression. Despite the dramatic radiographic appearance, serial neurological examinations demonstrated preserved motor function, intact sensation, and no bowel or bladder dysfunction (ASIA grade E).
Because the patient remained neurologically stable, the team pursued conservative management with close monitoring, rehabilitation restriction, serial imaging, and thrombosis prophylaxis without anticoagulation. The authors discuss several possible contributors to hematoma formation, including epidural venous bleeding, drainage management, blood pressure fluctuations, vascular fragility associated with advanced age, and postoperative hemodynamic changes unique to endoscopic spine surgery.
Follow-up MRI at 50 days demonstrated complete hematoma resolution with normalized thecal sac morphology. At 3-month and 6-month follow-up, the patient had minimal residual pain, preserved neurologic function, and no evidence of recurrent hematoma or cauda equina dysfunction.
This case is particularly notable because most postoperative spinal epidural hematomas presenting with neurological deterioration require emergent decompression within 6 hours to prevent permanent deficits. Here, however, a massive multilevel hematoma resolved completely without surgery, challenging assumptions regarding mandatory reoperation in carefully selected asymptomatic patients.
Why this case matters
- Describes an exceptionally rare five-segment postoperative epidural hematoma
- Demonstrates successful conservative management despite extensive imaging abnormalities
- Highlights the importance of neurological examination over imaging appearance alone
- Reinforces careful postoperative surveillance after UBE spine surgery
- Provides insight into pressure dynamics and bleeding mechanisms unique to minimally invasive endoscopic decompression
Clinical Take-Home Message
Extensive postoperative spinal epidural hematoma does not always mandate emergent surgical evacuation; in neurologically intact patients, carefully monitored conservative management with serial imaging and close neurological surveillance may achieve complete recovery.
Question:
What was the key factor supporting conservative rather than surgical management in this case?
A. Minimal hematoma size
B. Presence of severe canal compromise
C. Preserved neurological function without cauda equina syndrome
D. Early anticoagulation therapy
Correct answer: C. Preserved neurological function without cauda equina syndrome
Explanation:
Despite dramatic multilevel epidural hematoma extending from T12 to L4, the patient maintained intact motor, sensory, bladder, and bowel function (ASIA grade E). The absence of neurological deterioration allowed safe conservative management with serial monitoring.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in