After the paper | Guest post from Dr Danny Douek
Published in Microbiology

Research published by Douek and colleagues in the mid-2000s confirmed the involvement of the gut microbiome in the pathogenesis of HIV.
This post looks back at the 2006 paper 'Microbial translocation is a cause of systemic immune activation in chronic HIV infection' published in Nature Medicine. It's written by corresponding author Danny Douek, and is a story of generosity, collaboration and thinking outside the box.
To be perfectly honest, our paper showing that microbial translocation contributes to inflammation in HIV infection was met with some skepticism in the field. At least initially. Remember, this was in the days before the microbiome was “responsible for everything”.
The world of HIV pathogenesis was focused on the virus, the immune response to it, and homeostatic proliferation as key factors in the systemic immune activation that was recognized to be a critical driver of disease progression in both untreated and treated HIV disease.
The idea for microbial translocation came from three places. First, we and others had discovered the massive loss of CD4 T cells from the gut in acute HIV infection (although, to be honest again, this was actually a rediscovery of Don Kotler’s observations from the mid 1980s). Second, my work with bone marrow transplanters introduced me to the concept of the leakiness of a damaged gut. Third, Dirk van Bekkum’s experiments in gnotobiotic mice in the 1960s and those of Charlie Surh in the early 2000s clearly showed that to get homeostatic proliferation of T cells you need bacteria in the gut.
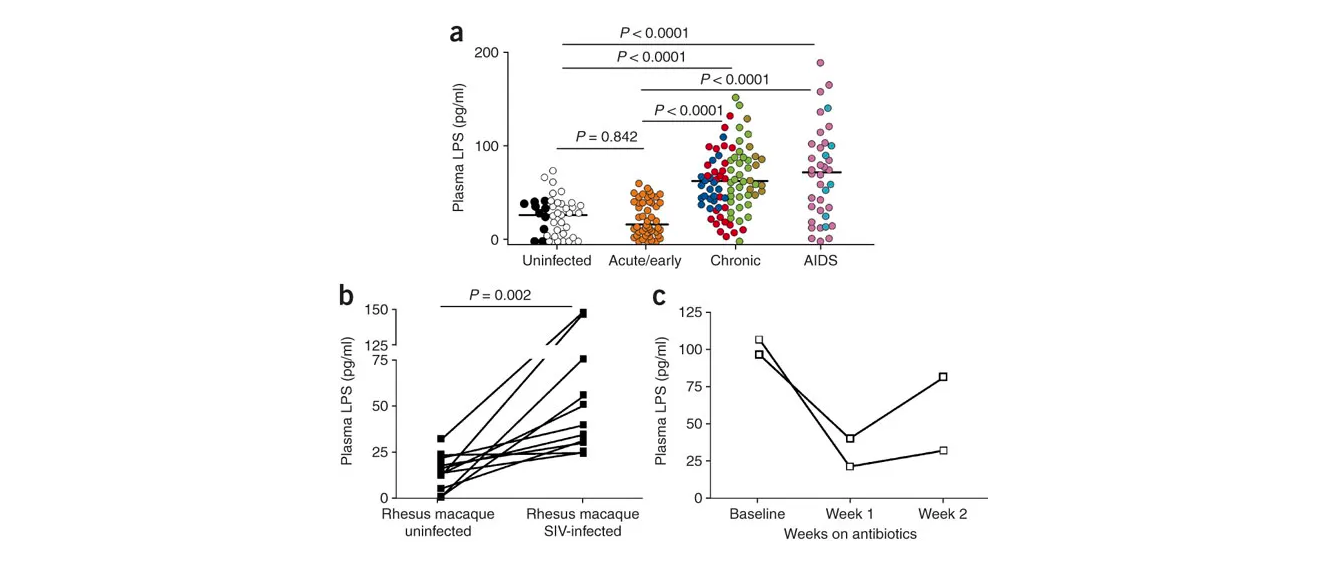
So, in the search for a cause of immune activation that persisted even when the virus load was brought down to undetectable levels with cART, we put these three ideas together and came up with a scenario in which the immunological and structural damage to the gut caused by the virus in acute infection increases gut permeability which allows microbial products to translocate into the circulation thereby causing systemic immune activation. And we measured it and there it was. Many other researchers subsequently reproduced our findings and the concept has now pretty much become mainstream, especially with the explosion of studies into the immunomodulatory effects of the microbiome.
I think our findings had an important impact on our approach to HIV disease and its management by contributing to a shift in focus away from the blood as an organ of study and towards the tissues, especially mucosal sites. They also emphasized the need to look at the system as a whole — the HIV-infected person — microbiome and all, in order to understand disease pathogenesis.
I too have learned many lessons from that experience, lessons that I try to impress upon younger scientists in my lab. First, I would have no work, no studies, no data and no papers if it were not for the HIV-infected people who so graciously provide tissue biopsies from their bodies that end up in tubes in my lab. Those of us who choose to study “human immunology” are sustained by the generosity of the humans whom we study and, by extension, the physicians and surgeons and nurses and coordinators who provide the infrastructure for our experiments. Second, collaborate with your friends — they will be honest enough to tell you that your idea is ridiculous but they may also have enough faith in you to give you their precious samples, time and skills. Finally, it’s important to look outside your field of expertise for inspiration.
I remember that after the paper came out, a friend of mine, a hepatologist gave me a wry smile, told me that our findings came as no surprise to him and he said: “We were wondering when you HIV people would figure that out…”.
(Poster image is Figure 1 from the paper)
Dr Danny Douek is chief of the Human Immunology Section at the Vaccine Research Centre.
Follow the Topic
-
Nature Medicine
This journal encompasses original research ranging from new concepts in human biology and disease pathogenesis to new therapeutic modalities and drug development, to all phases of clinical work, as well as innovative technologies aimed at improving human health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Clinical Research in Respiratory Medicine
Publishing Model: Hybrid
Deadline: Feb 18, 2027
Cancer Prevention and Control
Publishing Model: Hybrid
Deadline: Feb 19, 2027

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in