Autoimmune GFAP Astrocytopathy Misdiagnosed as Tuberculous Meningitis
Published in Neuroscience and Biomedical Research
Case report:
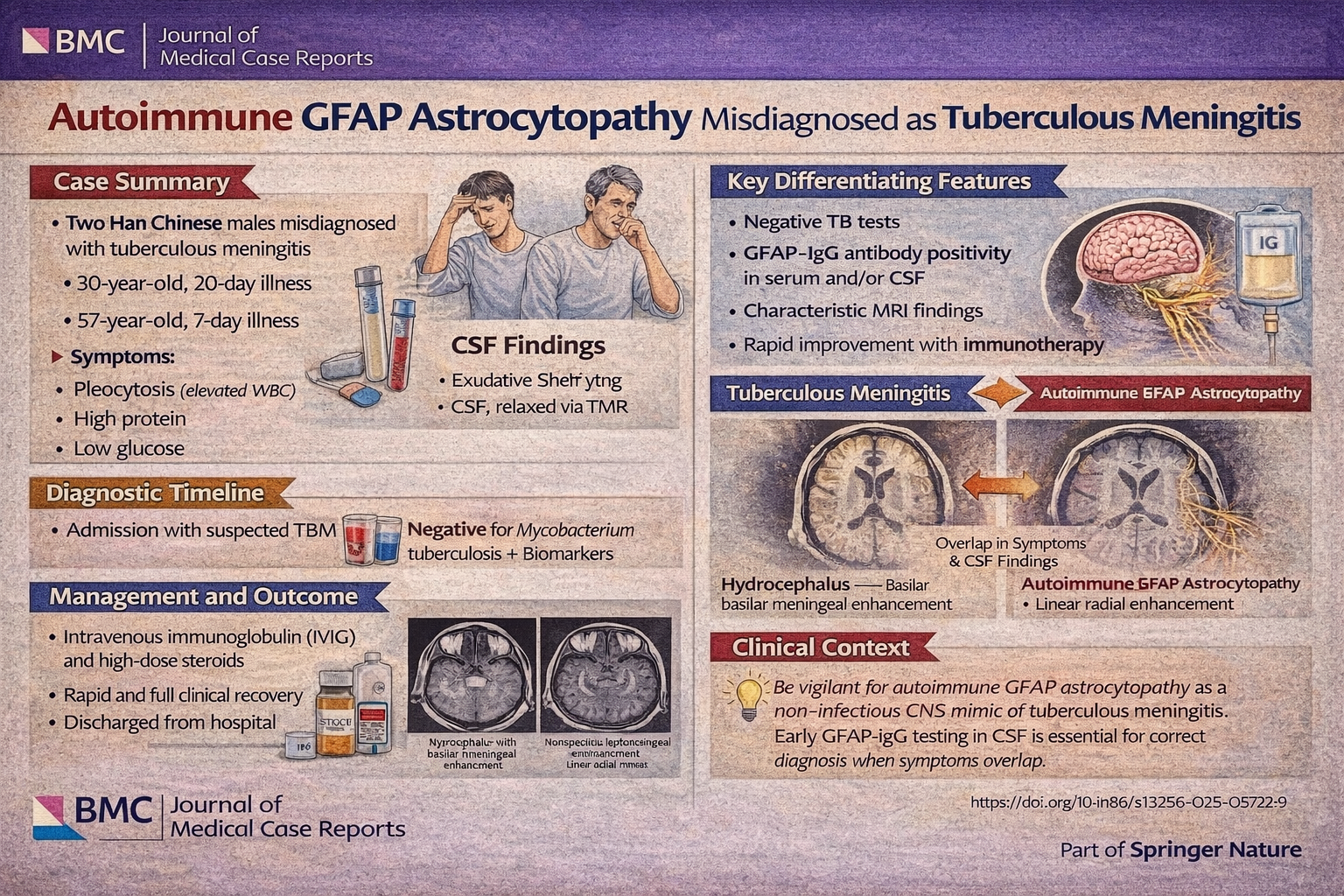
This case report describes two patients who were initially diagnosed with tuberculous meningitis based on a combination of subacute neurological symptoms, cerebrospinal fluid (CSF) inflammatory findings, and neuroimaging features consistent with infectious meningitis . Both individuals presented with clinical features highly suggestive of TBM, including headache, fever, and progressive neurological deficits, alongside CSF profiles demonstrating lymphocytic pleocytosis, markedly elevated protein, and reduced glucose or chloride levels. Magnetic resonance imaging further supported the presumed diagnosis, revealing diffuse leptomeningeal enhancement. In one case, a positive T-SPOT test reinforced diagnostic anchoring toward tuberculosis. However, despite appropriate antimicrobial and antituberculous therapy, both patients exhibited clinical worsening or failed to improve, prompting reconsideration of the initial diagnosis.
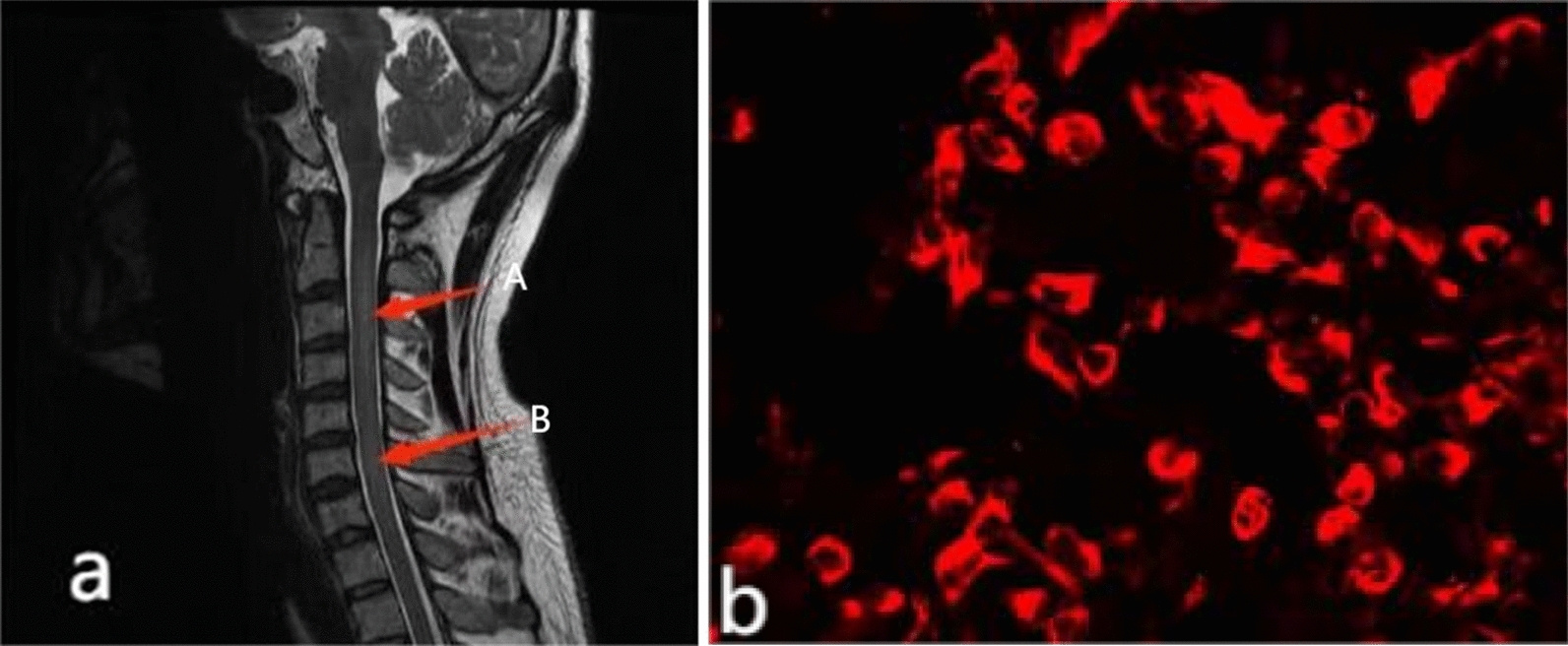
Subsequent evaluation revealed the presence of glial fibrillary acidic protein immunoglobulin G (GFAP-IgG) antibodies in the CSF and/or serum, leading to the diagnosis of autoimmune GFAP astrocytopathy. Clinically, the cases highlight the heterogeneity of this condition: one patient developed prominent cerebellar ataxia with meningoencephalomyelitis and optic involvement, while the other exhibited systemic symptoms including fever and tremor, along with autonomic dysfunction such as urinary retention. Notably, both patients developed hyponatremia during the disease course, an underrecognized but reported feature of GFAP astrocytopathy. Radiologically, although leptomeningeal enhancement overlapped with TBM, the broader pattern of central nervous system involvement—including spinal cord abnormalities—supported an inflammatory autoimmune process.
From a mechanistic standpoint, GFAP astrocytopathy is believed to be a T-cell–mediated autoimmune disorder, with GFAP antibodies serving primarily as biomarkers rather than direct pathogenic agents. The disease preferentially affects GFAP-rich regions, including the meninges, periventricular white matter, brainstem, and spinal cord. Importantly, both patients demonstrated significant clinical improvement following initiation of immunotherapy with high-dose corticosteroids and intravenous immunoglobulin, underscoring the critical importance of early recognition. These cases emphasize that autoimmune GFAP astrocytopathy can closely mimic tuberculous meningitis across clinical, laboratory, and imaging domains, and should be strongly considered in patients with presumed infectious meningitis who fail to respond to standard antimicrobial therapy.
Clinical Take-Home Message (Pearl):
In patients with presumed tuberculous meningitis who fail to improve—or who exhibit atypical features—early testing for CSF GFAP-IgG is essential, as timely recognition of autoimmune GFAP astrocytopathy allows for effective immunotherapy and prevents prolonged morbidity.
Question:
Which feature most strongly favors autoimmune GFAP astrocytopathy over tuberculous meningitis?
A. CSF lymphocytic pleocytosis
B. Leptomeningeal enhancement on MRI
C. Positive T-SPOT test
D. GFAP-IgG antibodies in CSF
Answer: D
CSF inflammation and imaging findings overlap significantly between TBM and GFAP astrocytopathy. Even TB-related tests may be misleading. GFAP-IgG positivity—especially in CSF—is the most specific diagnostic marker, identifying an autoimmune process that responds to steroids and immunotherapy rather than antimicrobials.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in