When One Hand Acts on Its Own: A Stroke Presentation with Mixed Alien Hand Features
Published in Neuroscience and Biomedical Research
Explore the Research
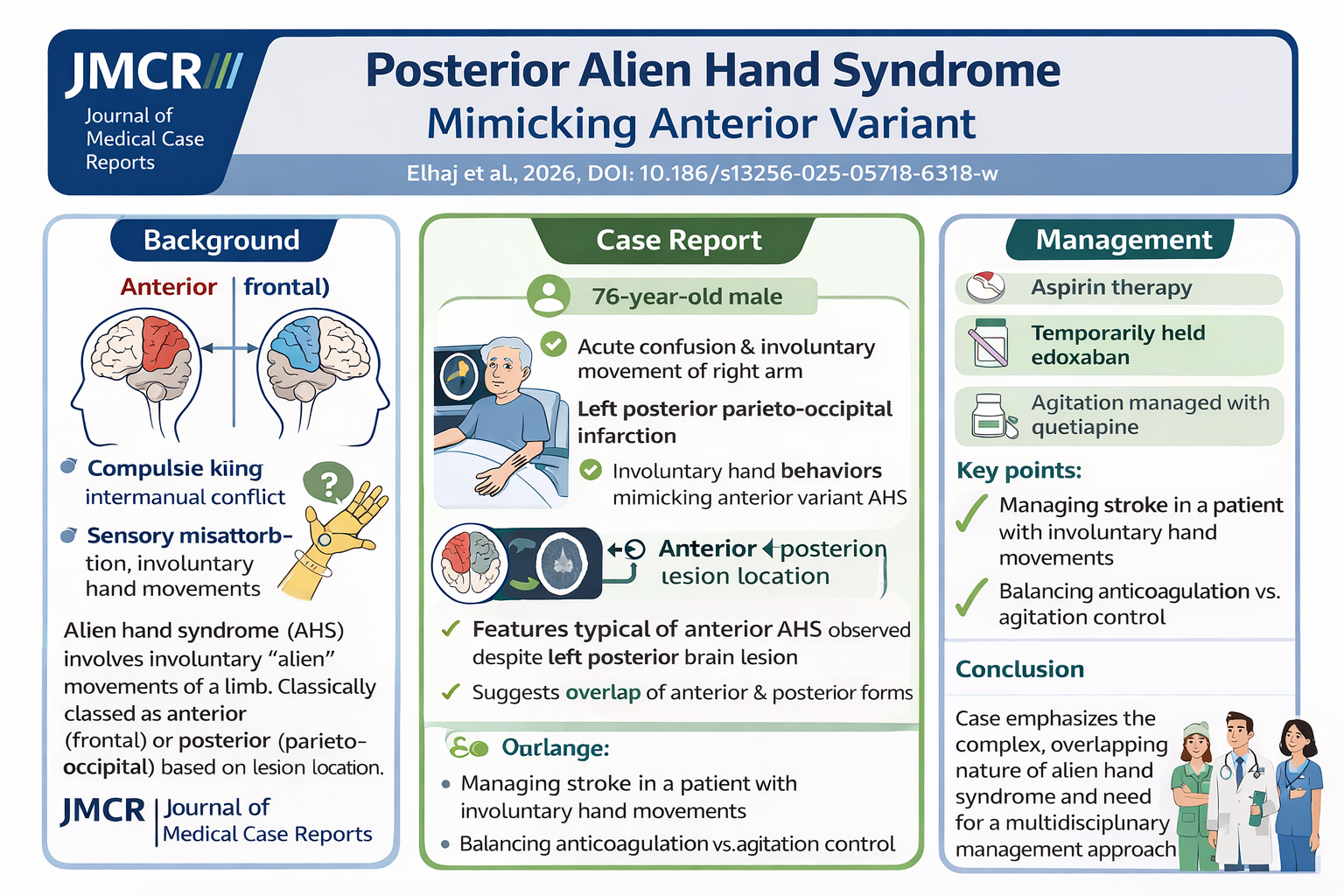
Posterior alien hand syndrome in a patient with parieto-occipital infarction: a presentation mimicking anterior variant features—a case report
Case Summary
A 76-year-old man presented with acute confusion and involuntary movements of his right arm following a fall. Initial imaging was unrevealing, but rapid clinical progression prompted repeat imaging, which demonstrated a left posterior circulation infarction .
The patient developed classic features of alien hand syndrome—autonomous limb activity perceived as foreign—yet with a posterior lesion producing features typically associated with anterior variants. This diagnostic overlap is particularly instructive.
Management required careful balancing of competing priorities:
Acute stroke treatment with antiplatelet therapy
Temporary cessation and later reintroduction of anticoagulation
Symptom control of involuntary movements and agitation (quetiapine)
The case illustrates the complex interplay between neuroanatomy, behavior, and stroke management, especially in patients with competing thrombotic and hemorrhagic risks .
Why This Case Matters
This report challenges the traditional dichotomy of AHS into strictly anterior vs posterior forms. Instead, it supports a network-based model, where disconnection across distributed cortical and subcortical regions produces hybrid clinical phenotypes.
Key implications
AHS can evolve dynamically with lesion progression
Posterior lesions may produce “anterior-like” behavioral manifestations
Early imaging may be falsely reassuring—clinical evolution should drive repeat imaging
Clinical Pearl
Alien hand syndrome should be viewed as a network disconnection syndrome—not a strictly localization-bound entity.
Question
Which mechanism best explains alien hand syndrome?
A. Primary motor cortex hyperexcitability
B. Peripheral nerve hyperactivity
C. Disconnection between motor planning and execution networks
D. Basal ganglia dopamine deficiency
Correct Answer: C
Explanation:
Alien hand syndrome arises from disrupted integration between intention (frontal/parietal networks) and motor execution pathways, often due to lesions affecting interhemispheric or frontoparietal connectivity. This disconnection leads to goal-directed movements that are not perceived as self-generated.
Final Thoughts
This case reinforces a principle that remains as relevant today as ever: neurology is best understood through networks, not isolated lesions. As imaging advances, our clinical frameworks must evolve accordingly.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access, and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in