Auxiliary Diagnosis of Papillary Thyroid Carcinoma Based on Spectral Phenotype
Published in Cancer

Thyroid cancer is currently the malignancy with the highest growth rate. Since 2000, various types of cancers have exhibited an upward trend, with thyroid cancer ranking first in terms of incidence growth rate. The incidence rates of all types of thyroid cancer have shown an increase and continue to display an upward trend [1,2]. Particularly in urban areas, the incidence rate among women is nearly three times that of men. Thyroid cancer has risen to the fourth position among newly diagnosed cancers in women, emerging as the rapidly escalating disease among solid tumors in the female population. It poses a significant threat to women's health, and the severity of its impact should not be underestimated [3].
How to apply a simple and fast examination method to clarify the nature of thyroid tumor was the question our group thought about. At that time, the group undertook the Anhui Province Key Research and Development Program project "Analysis of pathological characteristics of BRAF and RAS gene mutations on multifocal thyroid carcinoma and study of molecular mechanism", and found that most papillary thyroid carcinoma (PTC) had a good prognosis, but a small proportion still showed aggressive behavior [4,5]. Also, despite the good prognosis of PTC, 10%-15% of patients still have recurrence, and some of them have treatment difficulties. Factors other than BRAF mutations are thought to influence the aggressive clinical phenotype observed in the subgroup of PTC patients with this genetic alteration [6,7].
The application of thyroid aspiration cytology combined with BRAF-V600 gene testing is a reliable means of thyroid tumor diagnosis. Due to various conditions, intraoperative freezing examination is the mainstream means of diagnosing thyroid tumor classification applied in most primary units in China at present. Meanwhile, ultrasonography, radioactive iodine scan, CT scan and MRI scan among imaging diagnostic methods can also judge thyroid tumors, but imaging diagnosis, as an indirect diagnostic method, has a relatively high misdiagnosis rate for general thyroid diagnosis. Intraoperatively, the methods with higher diagnostic accuracy include intraoperative frozen diagnosis, pathological section analysis, and Braf genetic testing. The above methods have problems such as cumbersome operation process and long clinical waiting time, which greatly restrict the optimization of surgical plan. Meanwhile, due to the existence of delayed diagnosis, patients sometimes often have to undergo reoperation, which increases the physical and psychological burden of patients and the workload of hospitals.
The researchers from the School of Communication and Electronic Engineering at East China Normal University and their collaborators explored the feasibility of applying spectroscopic techniques for rapid intraoperative aid in diagnosis of PTC. Our group constructs a thyroid cancer classification model by combining spectral data with feature space optimization method, combines image analysis, signal processing, machine learning and other techniques in the field of information science to extract strongly correlated mapping features, constructs a mapping feature dataset for thyroid cancer, introduces a multivariate space optimization method, and finally constructs a thyroid cancer classification model based on mapping union and feature space optimization. The distribution of the selected spectral features of thyroid cancer is shown in Figure 1.
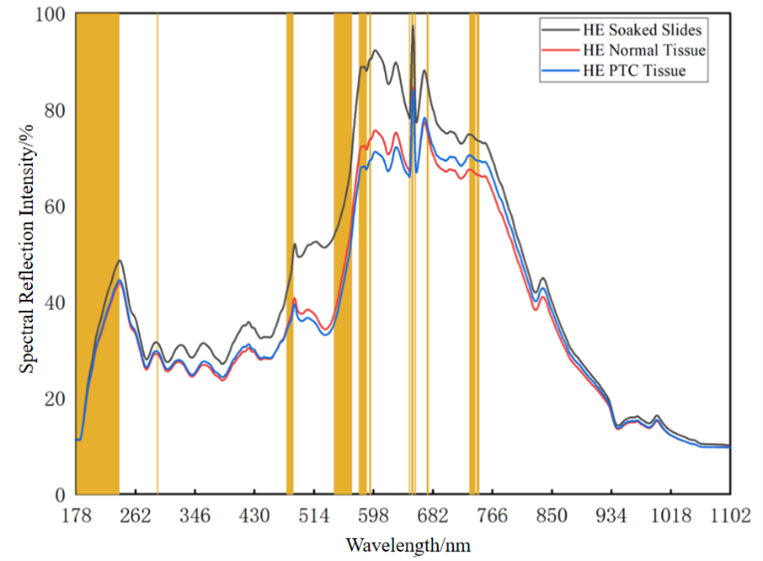
Figure 1 Characteristic wavelength distribution. HE soaked slide refers to the stained slide without samples; HE normal tissue refers to the slide with stained normal thyroid tissue; and HE PTC tissue refers to the slide with stained PTC tissue.
The correlation representation of the spectral and spatial features is shown in Figure 2. The model has a certain degree of interpretability from the perspective of pathological images and clinical applications, which shows a moderate correlation with the cell arrangement structure, average nucleus size and free thyroxine (FT4) at 188-228 nm, and a strong correlation with triiodothyronine (T3) at the maximum correlation index. The absorption peaks of oxyhemoglobin and most amino acids are present at the maximum correlation index (208 nm, 210 nm, 219 nm).
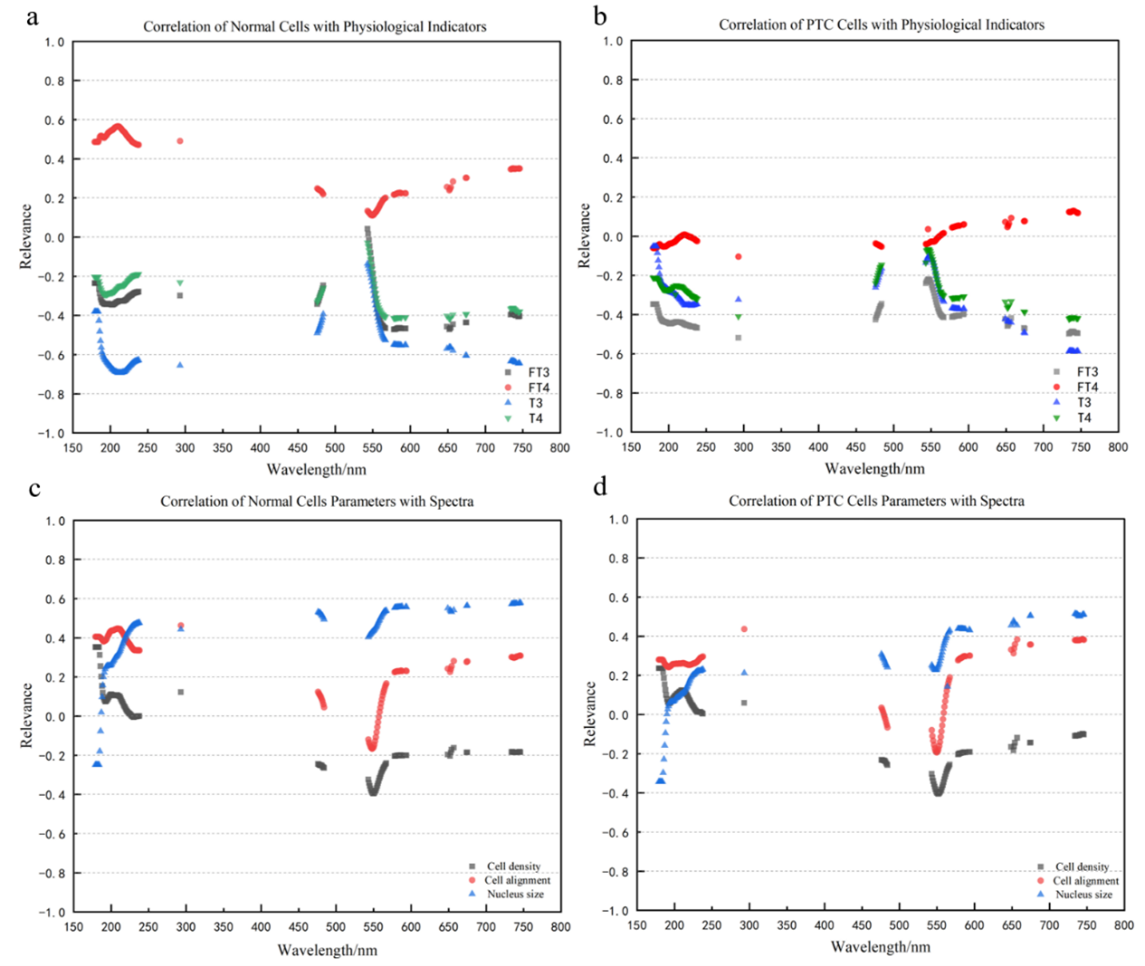
Figure 2 Correlation diagram. a Correlation of normal cell spectra with physiological indicators, b Correlation of PTC cell spectra with physiological indicators, c Correlation of normal cells parameters with spectra, d Correlation of PTC cells parameters with spectra.
In this study, we have conducted preliminary exploration of the application of spectral phenotyping in the pathological detection of PTC during surgery. The spectral acquisition device used in this study is shown in Figure 3. In subsequent research, the approach of utilizing spectral phenotyping to investigate material characteristics can be extended to the study and detection of other types of tumors. However, during practical application, we have found that the quality of the acquired spectra can be affected by various factors, such as the difference in sample preparation (for example, the amount of solution used, the thickness of sample slice, and the depth of the slice color), the variability of the sample itself (For example, calcification of the thyroid gland), the accuracy and stability of spectral acquisition equipment, the difference between the size of the spectral acquisition region and the tumor area, and the difference between the optical fiber collection area and the required area. These factors can introduce variability and uncertainty in the spectral data, and thus, the model performance is affected. Therefore, in further research, we will continue to explore and optimize the spectral acquisition process to improve the quality and reliability of the spectral data. This will enable a better application of spectral phenotyping in tumor research and clinical detection, providing a reliable basis for accurate diagnosis and treatment.
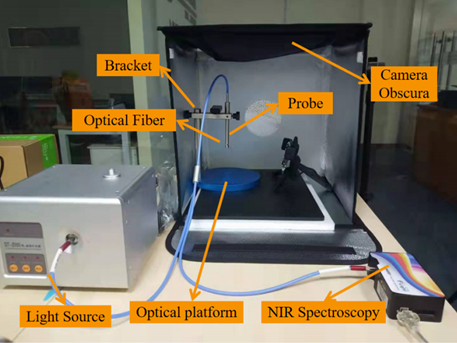 Figure 3 Self-built spectra acquisition device.
Figure 3 Self-built spectra acquisition device.
References
[1] Wen J, Yin CY, Liao GW, et al. Application of GM (1,1) Model in Predicting the Incidence Trend of Thyroid Cancer in China. Modern Oncology, 2022, 30(05): 899-902.
[2] Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid, 2016, 26(1): 1-133.
[3] Siegel Rebecca L, Miller Kimberly D, Jemal Ahmedin. Cancer Statistics, 2019. CA: A Cancer Journal for Clinicians, 2019, 69(1): 7-34.
[4] Geng L, Wang S, Zhao Y, et al. Gene Expression Profile in Mouse Bacterial Chronic Rhinosinusitis. Experimental and Therapeutic Medicine, 2019, 17(5): 3451-3458.
[5] Baloch ZW, Asa SL, Barletta JA, et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocrine Pathology 2022, 33(1): 27-63.
[6] Xing M, Liu R, Liu X, et al. BRAF V600E and TERT Promoter Mutations Cooperatively Identify the Most Aggressive Papillary Thyroid Cancer with Highest Recurrence. Journal of Clinical Oncology, 2014, 32(25): 2718-2726.
[7] Liu X, Qu S, Liu R, et al. TERT Promoter Mutations and Their Association with BRAF V600E Mutation and Aggressive Clinicopathological Characteristics of Thyroid Cancer. Journal of Clinical Endocrinology and Metabolism, 2014, 99(6): E1130-1136.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in