Biomedical consequences of elevated cholesterol-containing lipoproteins and apolipoproteins on cardiovascular and non-cardiovascular outcomes
Published in Healthcare & Nursing

Blood lipids, lipoproteins and cardiovascular disease
The circulating blood lipids mainly comprise triglyceride (TG) and cholesterol. These are insoluble in water and must be transported within membrane bound lipoprotein particles (lipoproteins) which also contain certain proteins with enzymatic or targeting function. Lipoproteins play a key role in dietary lipid transport and absorption by the small intestine, in the transport of lipids from liver to tissues, and the transport of lipids from peripheral tissues to the liver and intestine (reverse cholesterol transport)1. The main lipoprotein groups are traditionally divided into seven classes, categorised based on the relative densities of the aggregates from ultracentrifugation as; chylomicrons (CMR), CMR remnants, very-low density lipoproteins (VLDL), intermediate density lipoproteins (IDL), low-density lipoproteins (LDL), high-density lipoproteins (HDL), and Lp (a). Chylomicron remnants, enriched in cholesterol are considered to be pro-atherogenic. Very-low density lipoproteins produced by the liver are TG-rich and contain one core structural ApoB-100 molecule. VLDL, VLDL-remnants and IDL particles that are enriched in cholesterol and contain the ApoB-100 isotope and ApoE. As most TG has been removed, the lipoprotein becomes denser and is referred to as a low-density lipoprotein (LDL) that contains one ApoB-100 molecule carrying most of circulatory cholesterol. HDL play an important role in reverse cholesterol transport from peripheral tissues to the liver, which is considered one of the potential mechanisms by which HDL may be anti-atherogenic1,2.
Observational and randomised studies spanning the last three decades have convincingly demonstrated the association of higher concentrations of LDL-cholesterol and increased coronary heart disease risk. As a result, LDL-cholesterol lowering using statins form the mainstay of CVD prevention in the clinic. In contrast, while the non-randomised evidence suggests a relationship between total triglyceride concertation, HDL-cholesterol concentrations and, CHD risk, there is a marked absence of successful drug trials targeting these blood lipids showing any clinical CVD benefit3.
Lipid lowering drugs affect lipid concentrations beyond the LDL fraction. It is possible that both TG and cholesterol in lipoprotein subfractions play a causal role in disease progression or, that one lipid dominates and accounts for the relationship of any particular lipoprotein subfraction with CHD. Advances in NMR spectroscopy now allow interrogation of the lipid content (both cholesterol and TG) of each lipoprotein subfraction individually. For example, it is possible to measure both the cholesterol and TG content of IDL. This provides new opportunities to explore relationships of individual lipoprotein subfractions and both their TG and cholesterol content on CHD risk. By identifying genetic variants that associate with individual lipoproteins and their TG or cholesterol content, it also becomes possible to investigate whether any such relationships are causal using Mendelian randomisation (MR), while recognising certain limitations to this approach3,4.
Mendelian Randomisation - what in the Gregor Mendel is the point of the method?
Mendelian randomisation analysis is facilitated by genome-wide association studies (GWAS). The fundamental principle of MR analysis and from which the name ‘Mendelian randomisation’ is derived, is in reference to Mendel’s Second Law on the independent random assortment of alleles during meiosis, where DNA is transferred from parent to offspring at the time of gamete formation. Inheritance of a particular variant or group of variants in an individual’s DNA is inherited independent of other characteristics4,5. The valuable advantages of MR studies over observational studies are that genetic variants used as instrumental variables in MR studies are not susceptible to reverse causality, are not subjective to confounding due to Mendel’s second law, and are measured with precision, reducing regression dilution bias due to measurement error. The application of publicly available genetic data used in MR studies to evaluate relationship between risk factor-disease outcomes has made it a powerful tool in determining causal inference6,7.
What did we do in this study?
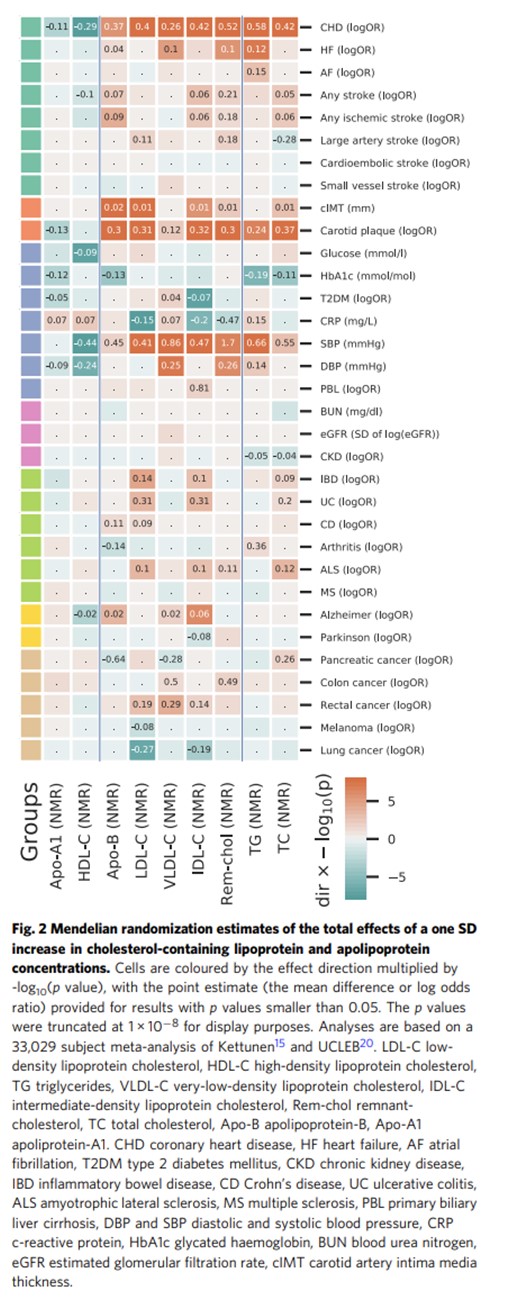
In this paper, we use genetic associations on NMR-measured metabolites and apply two-sample MR to determine the causal relevance of the cholesterol content on different lipoprotein subfractions on a range of cardiovascular (CVD) outcomes, disease biomarkers, measures of organ or systems function as well as late-in-life non-CVD conditions. We then perform multivariable MR to investigate whether causal effects might be independent of the routinely measured blood lipids LDL-C, HDL-C, and TG.
We find that the cholesterol content of a range of lipoprotein subfractions associate with atherosclerosis, biomarkers and CHD. Many of the effects act independently of LDL-cholesterol and may support the targeting of holistic lipid perturbation across multiple lipoproteins for disease prevention.

- Libby, P. et al. Atherosclerosis. Nat. Rev. Dis. Prim. 5, 1–18 (2019).Ross, R. Cell biology of atherosclerosis. Annu. Rev. Physiol. 57, 791–804 (1995).
- Weber, C. & Noels, H. Atherosclerosis: Current pathogenesis and therapeutic options. Nature Medicine vol. 17 1410–1422 (2011).
- Nordestgaard, B. G. Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: New Insights From Epidemiology, Genetics, and Biology. Circ. Res. 118, 547–63 (2016).
- Bennett, D. A. & Holmes, M. V. Mendelian randomisation in cardiovascular research: an introduction for clinicians. Heart 103, 1400–1407 (2017).
- Hingorani, A. & Humphries, S. Nature’s randomised trials. Lancet (London, England) 366, 1906–8 (2005)
- Hingorani, A. D. et al. Improving the odds of drug development success through human genomics: modelling study. Sci. Rep. 9, 18911 (2019).
- Schmidt, A. F. & Dudbridge, F. Mendelian randomization with Egger pleiotropy correction and weakly informative Bayesian priors. J. Epidemiol. 47, 1217–1228 (2018).
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Exercise and Physical Activity in Health and Disease
Publishing Model: Open Access
Deadline: Sep 03, 2026
Life Course Epidemiology
Publishing Model: Open Access
Deadline: Sep 30, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in