Cracking the “Seed and Soil” Code in Lung Adenocarcinoma Metastasis – A Spatial Transcriptomics Journey
Published in Biomedical Research
As oncologists, we face a heartbreaking reality every day: once lung adenocarcinoma (LUAD) spreads to distant organs, treatment options shrink dramatically and outcomes worsen. Even more puzzling, the same type of lung cancer can “choose” different destinations – brain, liver, adrenal glands, or bones. Why?
Back in 1889, surgeon Stephen Paget proposed the famous “seed and soil” hypothesis: cancer cells (the seeds) only grow in certain organs (the soil) that suit them. Yet more than a century later, we still struggle to predict at diagnosis: where will this patient’s cancer metastasize? How long will they survive after metastasis? Which therapy might work?
These clinical questions drove our team to launch this study.
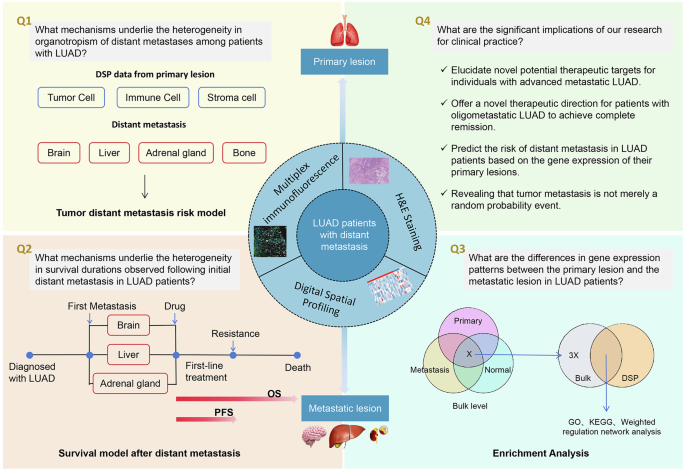
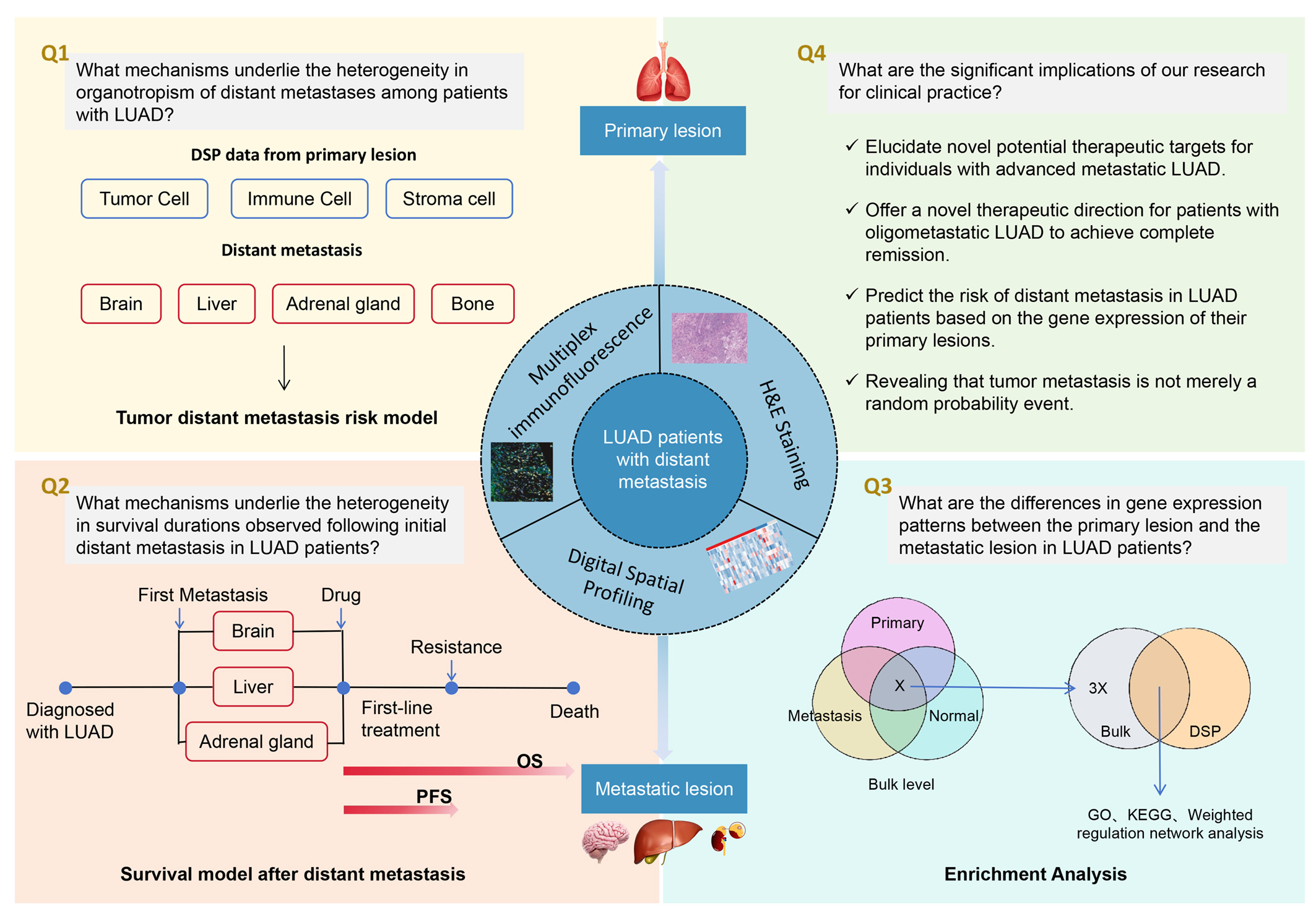
Mapping the microscopic landscape
Traditional genetic tests grind tumor tissue into a pulp – losing all spatial information. But a tumor is not a uniform soup. Cancer cells, immune cells, and stromal cells talk to each other in specific neighborhoods. That spatial dialogue is key to metastasis.
We used a cutting-edge technique called Digital Spatial Profiling (DSP). Think of it as drawing a detailed map of each tumor sample. Under the microscope, we marked three distinct areas: “tumor” regions (dense cancer cells), “immune” regions (immune cell hotspots), and “stromal” regions (connective tissue). Then we collected gene expression data from each area separately. This way, we didn’t just know which genes were active – we knew exactly where they were speaking.
Our team enrolled 52 patients with advanced LUAD. We collected matched samples of primary tumors and their metastases: 23 brain, 26 liver, and 3 adrenal gland pairs. We also performed multiplex immunofluorescence (mIF) to quantify over 20 immune cell types.
Four organs, four prediction keys
Our most exciting finding: the primary tumor’s molecular signature already “encodes” where it will metastasize. Using machine learning (random forest models), we built risk prediction tools for brain, liver, adrenal, and bone metastases – all with AUC values above 0.9. That means from the primary tumor alone, we can predict organ-specific metastasis risk with remarkable accuracy.
Take brain metastasis. The model flagged key genes like FKBP1A (in cancer cells), AFAP1L1 (in immune cells), and CKAP2 (in stromal cells). Surprisingly, pathways linked to cell death were strongly enriched in high-risk primary tumors. This suggests that cancer cells destined for the brain are already pre-equipped to resist death – a survival advantage that helps them travel through the bloodstream and colonize the brain.
Liver metastasis told a different story. Histone genes (H3C13, H4C12) and ribosomal protein genes (RPL36A, RPL38) were widely upregulated after metastasis. This hints at a “dormancythenreawakening” strategy: liverseeking cancer cells remodel their chromatin and protein synthesis machinery to adapt to the liver’s unique metabolic environment.
Adrenal and bone metastases had their own unique gene signatures. Interestingly, bone metastasis showed no single pathway enrichment – suggesting its propensity may stem from broad, fundamental biological processes rather than one specific switch.
The immune system’s doubleedged sword
Using mIF, we quantified over 20 immune cell types. In metastatic lesions, higher infiltration of M2 macrophages (usually protumor and immunosuppressive) correlated with longer overall survival. This challenges the conventional view. We interpret this cautiously – it may be influenced by tissue repair responses after systemic therapy, or by other confounding factors. But it certainly tells us that the immune story is far more nuanced than we thought.
HEindex: a simple but powerful metric
We also introduced a new parameter called the HEindex, derived from routine H&E stains. Using the digital pathology platform, we measured the average proportion of nontumor cells (immune or stromal) within 20 micrometres of each tumor cell. A higher HEindex means more contact between cancer cells and their surroundings.
Remarkably, a high HEindex in primary tumors was linked to higher adrenal metastasis risk, while a high HEindex in metastatic lesions was linked to better postmetastasis survival. This simple metric could become a practical biomarker available in any pathology lab.
From prediction to clinic: a twostage vision
Based on our findings, we propose a twostage clinical framework:
Stage 1 – At initial diagnosis: Use the primary tumour to generate four organspecific risk scores. Highrisk patients can receive tailored surveillance – for example, more frequent brain MRI for brainhigh risk, or early boneprotective agents for bonehigh risk. This allows earlier detection and intervention before overt metastasis.
Stage 2 – After metastasis occurs: If a patient already has a confirmed metastasis, our postmetastasis survival models (for PFS and OS) can help stratify patients. Lowrisk patients can continue standard therapy; highrisk patients (likely resistant to conventional treatment) could be offered clinical trials or functional precision medicine approaches, such as patientderived organoid drug testing.
Limitations and next steps
We must be honest about limitations. Our sample size was modest, especially for adrenal and bone metastases. We lack external validation cohorts. Functional experiments (gene editing, animal models) are still needed. And because bone metastasis samples are very hard to obtain, we could not build a survival model specifically for bone.
Final thoughts
What excites us most is not a single gene – but the proof of concept that a tumour’s metastatic destiny is already written in the spatial architecture of the primary lesion. By reading this “molecular map”, we may be able to predict the cancer’s travel route earlier than ever before, and offer patients more precise, proactive care.
Science is a marathon, not a sprint. Each small discovery brings us one step closer to making metastasis a predictable – and perhaps even preventable – complication.
Follow the Topic
-
Signal Transduction and Targeted Therapy
This is an international, peer-reviewed, open-access journal publishing articles related to signal transduction in physiological and pathological processes, alongside signal transduction-targeted therapeutics in the form of biological agents and small molecular drugs used to treat human diseases.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in