Impact of conditioning chemotherapy on lymphocyte kinetics and outcomes in LBCL patients treated with CAR T-cell therapy
Published in Cancer
The problem
Chimeric antigen receptor (CAR) T-cell therapy has revolutionized the treatment of hematologic cancers, particularly lymphoma. In this type of treatment, T cells are collected from the patient, modified in the laboratory to target tumor cells, and then infused back into the patient. When this technique was initially being developed, it was found that giving conditioning chemotherapy (CCT) before cell infusion improved the ability of the CAR T-cells to expand and kill the tumor1. However, the precise mechanisms by which CCT exerts this effect are still unclear. One thought is that CCT works primarily by eliminating host lymphocytes, thereby creating an appropriate “space” for the CAR T-cells to survive and proliferate – this is why CCT is frequently referred to as “lymphodepletion”.2 Other mechanisms related to elimination of sinks for homeostatic cytokines and eradication of immunosuppressive cells (such as myeloid-derived suppressor cells) also play a role.3,4
In the clinical setting, there is substantial variability between patients both in terms of their response to CCT and in terms of CAR T-cell efficacy. For instance, while patients who receive high-intensity CCT have a greater probability of achieving a favorable cytokine profile, high levels of IL-7 and IL-15 are associated with improved outcome independent of CCT intensity.5 To better understand this variability and the role that CCT plays in determining CAR T-cell efficacy, we decided to focus on a simple, intuitive clinical marker – the change in absolute lymphocyte count during CCT, which we referred to as the delta lymphocyte index (DLIx). In this study, we determined how the DLIx relates to clinical outcomes, cytokine levels and genetic variation in patients with large B-cell lymphoma (LBCL) receiving CAR T-cell therapy.
Our findings
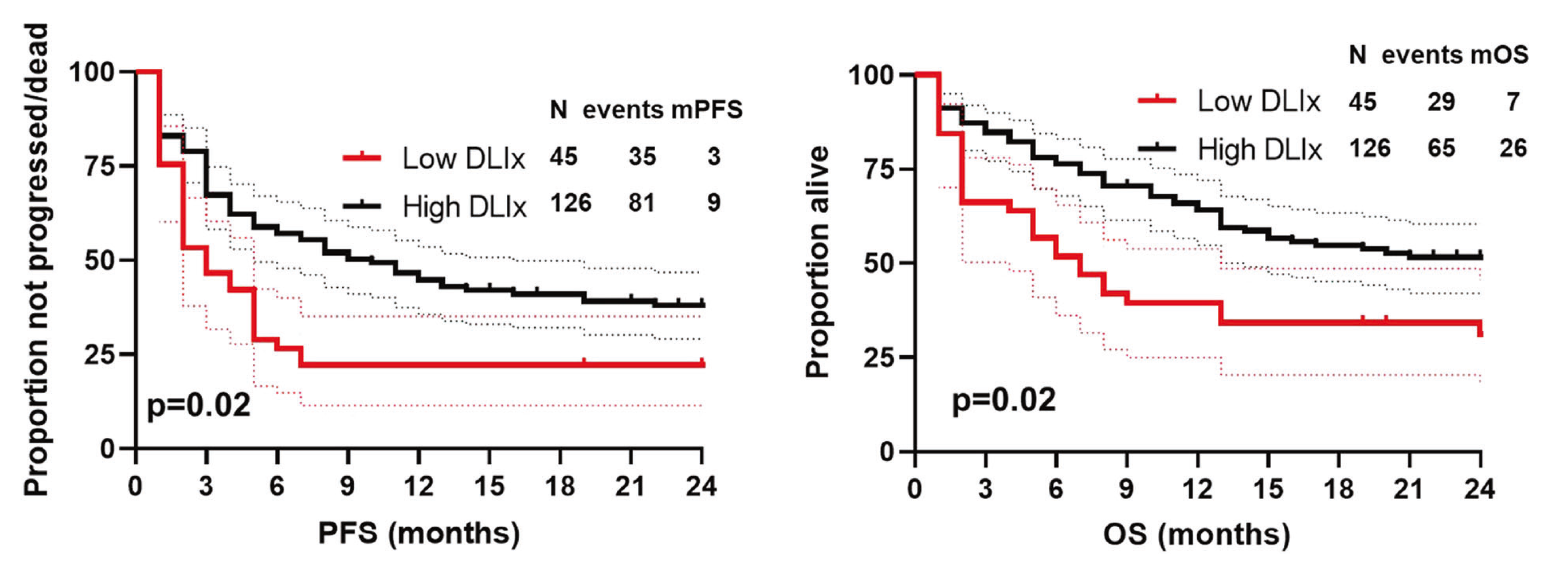
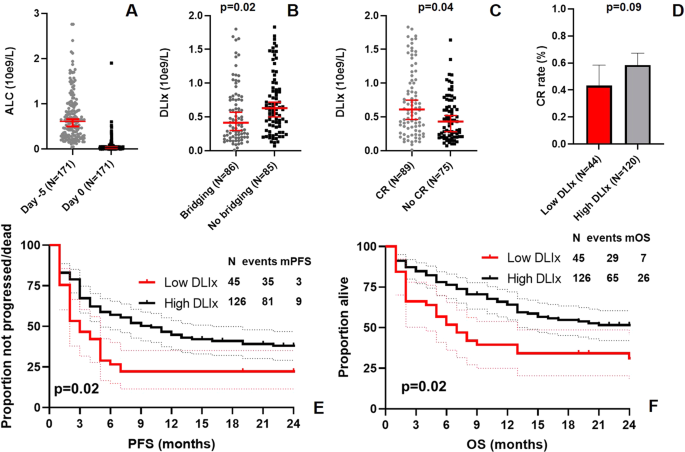
We studied 171 patients with relapsed or refractory LBCL treated with standard-of-care axicabtagene ciloleucel (axi-cel) at our institution, the University of Texas MD Anderson Cancer Center. DLIx was significantly higher in patients who achieved a complete response (CR) compared to those who did not, with a CR rate of 43% in patients with low DLIx and 58% in patients with high DLIx. The use of bridging therapy was significantly associated with low DLIx. Interestingly, low DLIx was independently associated with shorter progression-free (PFS) and overall survival (OS), even when accounting for other variables such as performance status, International Prognostic Index scores and use of bridging therapy (see Figure).
No significant differences in IL-7 or IL-15 levels were found between patients with low and high DLIx. However, we did find an association between DLIx and genetic variants involving three genes. The first gene (ABCB1) encodes for a well-known membrane efflux pump involved in chemotherapy metabolism and likely relates to pharmacokinetic differences between patients in terms of CCT metabolism. The other two genes (MISP and CPVL) play an important role in macrophage biology and suggest that macrophages may play a role in mediating the effect of CCT.
Figure

Take-away points
The DLIx is an easily calculated clinical marker describing the impact of CCT on lymphocyte count. We found that DLIx was affected by use of bridging therapy and that low DLIx was independently associated with inferior CR rate, PFS and OS in patients with LBCL receiving CAR T-cell therapy. The results of our genetic analysis suggest that macrophages may play a role in mediating the effect of CCT and support further studies aimed at investigating macrophage biology in this setting.
References
- Turtle CJ, Hanafi L-A, Berger C, et al. Immunotherapy of non-Hodgkin’s lymphoma with a defined ratio of CD8+ and CD4+ CD19-specific chimeric antigen receptor–modified T cells. Science Translational Medicine. 2016;8(355):355ra116-355ra116.
- Muranski P, Boni A, Wrzesinski C, et al. Increased intensity lymphodepletion and adoptive immunotherapy--how far can we go? Nat Clin Pract Oncol. 2006;3(12):668-681.
- Gattinoni L, Finkelstein SE, Klebanoff CA, et al. Removal of homeostatic cytokine sinks by lymphodepletion enhances the efficacy of adoptively transferred tumor-specific CD8+ T cells. J Exp Med. 2005;202(7):907-912.
- Wrzesinski C, Paulos CM, Kaiser A, et al. Increased intensity lymphodepletion enhances tumor treatment efficacy of adoptively transferred tumor-specific T cells. Journal of immunotherapy (Hagerstown, Md : 1997). 2010;33(1):1-7.
- Hirayama AV, Gauthier J, Hay KA, et al. The response to lymphodepletion impacts PFS in patients with aggressive non-Hodgkin lymphoma treated with CD19 CAR T cells. Blood. 2019;133(17):1876-1887.
Follow the Topic
-
Leukemia
This journal publishes high quality, peer reviewed research that covers all aspects of the research and treatment of leukemia and allied diseases. Topics of interest include oncogenes, growth factors, stem cells, leukemia genomics, cell cycle, signal transduction and molecular targets for therapy.





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in