Lung involvement in rheumatoid arthritis: what do we know?
Published in Public Health

Rheumatoid arthritis (RA) is a highly prevalent heterogeneous group of immune-mediated inflammatory diseases with chronic and multisystemic physiopathogenesis involving several organs. Interstitial pneumonia has emerged as the most prevalent manifestation, affecting up to 60% of patients and, in some cases, preceding joint symptoms. The effectiveness of treatments varies, with specific disease-modifying antirheumatic drugs (DMARDs) showing potential for controlling pulmonary symptoms. Early diagnosis and tailored treatment strategies are crucial for the effective management of RA-related pulmonary diseases.
RA can affect all compartments of the thorax, including the pulmonary parenchyma, large and small airways, pleura, and, less frequently, vasculature. Lung involvement typically occurs approximately five years after the diagnosis of RA, and few respiratory symptoms may precede the onset of joint symptoms.
Interstitial lung disease (ILD) is the most common manifestation of pulmonary involvement, with a prevalence of up to 80% reported via biopsy. Some cases may progress to pulmonary fibrosis and subsequent respiratory insufficiency, with implications for disease prognosis. Unfortunately, the incidence of ILD is underestimated, especially in the early stages of subclinical disease. Other pulmonary manifestations include airway involvement, pleural involvement, and rheumatoid pulmonary nodules. The pulmonary toxicity caused by drugs used to treat RA itself, including DMARDs, whether synthetic, or biological immunomodulators or so-called small molecules, is highly relevant. Synthetic drugs, mainly methotrexate (MTX), sulfasalazine (SSZ) and leflunomide (LFN), have been implicated in the onset of respiratory manifestations. The use of immunobiological therapies, such as tumor necrosis factor inhibitors (anti-TNF), has also been associated with the development or exacerbation of ILD in patients with RA.
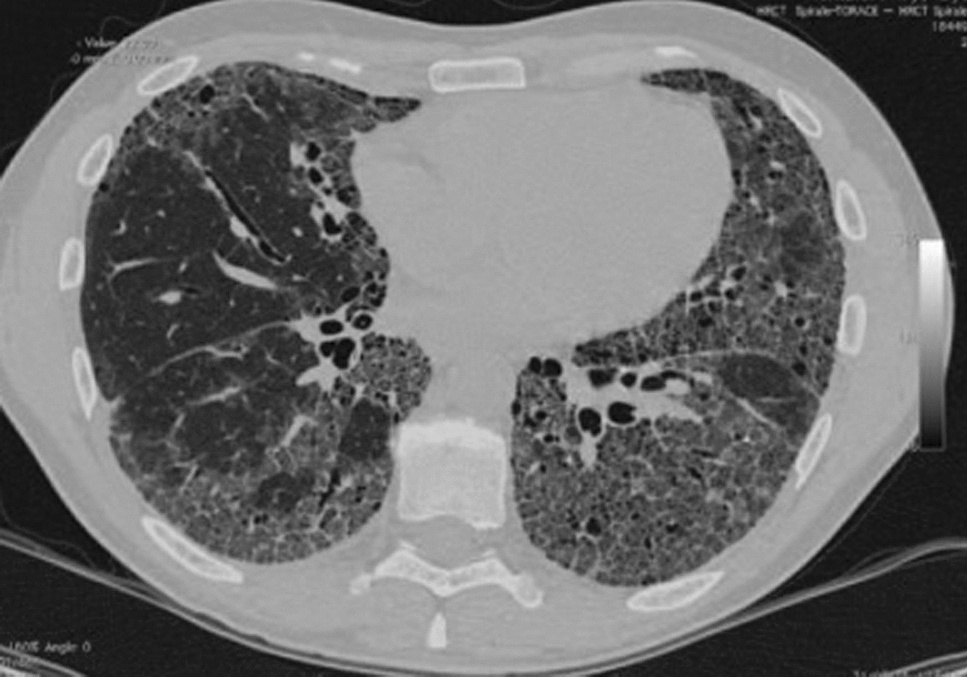
With more sophisticated radiological techniques, such as high-resolution computed tomography of the chest (HRCT), diagnosing pulmonary involvement in RA is more efficient, with tomographic findings predominating in approximately 55% of cases. HRCT identified interstitial pulmonary abnormalities and small airway involvement, most often in subclinical disease. The most common tomographic findings are the presence of pulmonary infiltrates with a predominance of ground-glass changes and septal and subpleural thickening, usually to a small extent.
Although RA is more common in women, ILD associated with RA (RA–ILD) occurs more frequently in men in the sixth decade of life. Some risk factors for developing RA–ILD are male sex, advanced age, smoking, high titers of antibodies to RF and/or anti-CCP, RA disease activity, decreased functional status, and the presence of other nonpulmonary extra-articular diseases, such as subcutaneous rheumatoid nodules. Genetic risk factors have also been identified in RA–ILD, including the MUC5B promoter variant particularly associated with the usual interstitial pneumonia (UIP) pattern and various rare variants in telomerase. Individuals with RA are nine times more likely to develop ILD than the general population. Only 10% of patients with RA–ILD exhibit respiratory symptoms.
Interstitial lung disease comprises a spectrum of histological types with different clinical and radiological patterns. There is a vast spectrum of pulmonary histopathology in ILD patients with RA, with classes according to the American Thoracic Society/European Respiratory Society classification system for idiopathic interstitial pneumonia. The most common histopathological types are usual interstitial pneumonia (UIP) , nonspecific interstitial pneumonia (NSIP), and organizing pneumonia (OP). Other patterns of pulmonary involvement in RA include macrophage interstitial pneumonia (desquamative), diffuse alveolar damage, and lymphocytic interstitial pneumonia.
Once the diagnosis of RA has been established, the therapeutic approach is defined based on the joint symptoms. Unlike systemic sclerosis, where lung involvement is strategically investigated before treatment is defined, screening strategies for RA–ILD are not implemented unless respiratory symptoms are present. Because there are no established screening strategies, many of these approaches have been extrapolated to treating scleroderma or interstitial pulmonary fibrosis (IPF). Pulmonary function tests and HRCT can be used as diagnostic measures, especially in patients with risk factors such as smoking and advanced age.
Because there is no completely established therapeutic approach, decisions should be based on the benefits and clinical presentation of each patient. In asymptomatic patients with nonprogressive ILD, treatment is conservative. There is no defined therapeutic approach and patients with UIP respond poorly to treatment. Patients with NSIP and OP patterns may respond more favorably to immunosuppressants; however, some patients present with mixed or unclassifiable patterns on HRCT, making disease progression and therapeutic response unpredictable.
Follow the Topic
-
Discover Medicine
This is a fully open access, peer-reviewed journal that supports multidisciplinary research and policy developments across the fields of medical and clinical science.

Related Collections
With Collections, you can get published faster and increase your visibility.
Advances in Cardiovascular Diagnostics, Interventional Therapies, and Arrhythmia Management
Cardiovascular diseases remain a major global health challenge worldwide, continuing to be a leading cause of morbidity and mortality despite substantial advances in prevention and treatment. In recent years, progress in cardiovascular diagnostics, interventional techniques, and arrhythmia management has significantly improved patient care; however, important challenges persist, including timely diagnosis, individualized risk stratification, optimization of interventional strategies, and long-term outcome improvement. These unmet needs highlight the necessity for continued innovation and multidisciplinary research efforts in cardiovascular medicine.
This Collection aims to highlight recent advances in cardiovascular diagnostics, interventional therapies, and arrhythmia management, with a focus on clinically relevant and translational research. We welcome submissions addressing interventional cardiology procedures, catheter ablation techniques, three-dimensional electroanatomical mapping, mechanisms of cardiac arrhythmias, cardiovascular imaging, acute coronary syndromes, and hypertension. Contributions that enhance understanding of disease mechanisms, improve procedural outcomes, or inform clinical decision-making are particularly encouraged.
By bringing together high-quality experimental, clinical, and translational studies, this Collection seeks to advance scientific knowledge, support the development of improved therapeutic strategies, and foster global collaboration in the field of cardiovascular medicine.
Keywords:
Cardiology; Arrhythmia; Ablation; 3D mapping; Interventional cardiology; Hypertension; Acute coronary syndrome; Cardiovascular imaging; COVID-19
Publishing Model: Open Access
Deadline: Oct 12, 2026
Management of Breast Cancers in the Era of Artificial Intelligence
We are witnessing a full bloom of artificial intelligence (AI) in this day and age. The application of AI has been widely evaluated in different areas. One particular area is Oncology. Breast cancer is currently one of the commonest female cancers worldwide. Due to the intrinsic disease heterogeneity, tailored treatment with multi-disciplinary approach is the key to a successful treatment. AI has been considered as a potential tool to improve diagnostic and treatment outcomes of breast cancers.
This collection aims to compile good research articles evaluating the use of AI in the management of breast cancers. Potential topics include, but not limited to
1. AI in breast imaging
2. AI in breast pathology
3. AI in treatment decision making
4. AI in patient counselling
5. AI in breast cancer prognostication
Keywords:
1. Breast cancer
2. Breast oncology
3. Artificial Intelligence
4. Deep learning
5. Machine learning
Publishing Model: Open Access
Deadline: Dec 20, 2026





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in