Sex differences for clinical correlates of nigral loss in Lewy body disease
Published in Neuroscience and General & Internal Medicine

Lewy body dementia, including both Parkinson’s disease dementia and dementia with Lewy bodies, is defined by underlying Lewy body pathology and cognitive decline that impacts daily life. Although Lewy body dementia is the second most common type of neurodegenerative dementia following Alzheimer’s, research continues to be substantially scarce in this dementia compared to Alzheimer’s. While sex differences consistently get reported in Alzheimer’s, sex differences in Lewy body dementia are still not clearly understood and needs more investigations.
Autopsy studies so far showed females are not as likely as males to have pure Lewy body pathology, and have a higher likelihood for other pathologies accompanying Lewy body pathology (e.g., Alzheimer’s pathology). Having additional pathologies with Lewy body pathology lowers the likelihood of having a Lewy body dementia phenotype. However, our previous work showed that even when females have pure Lewy body pathology, they continue to be less likely to have a Lewy body dementia phenotype. Adding Alzheimer’s pathology to the mix showed that females continue to be less likely than males to have a Lewy body dementia phenotype when comparing females and males with similar levels of Lewy body and Alzheimer’s pathology. So, building up on these previous studies we performed using the National Alzheimer’s Coordinating Center data, we wanted to look into the clinical correlates of substantia nigra neuron loss, the third pathology feature mentioned in the Lewy body dementia diagnosis.
Nigral loss has been associated with parkinsonism in people with Lewy body dementia. Although not every person with Lewy body dementia has nigral loss, it increases the likelihood of someone having a Lewy body dementia phenotype when it occurs given associations with parkinsonism. Females are less likely than males to have parkinsonism in Lewy body dementia. Thus, we wondered if nigral loss contributes to this sex difference.
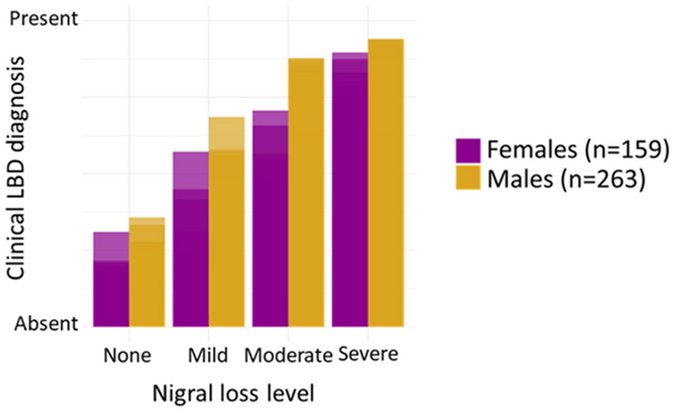
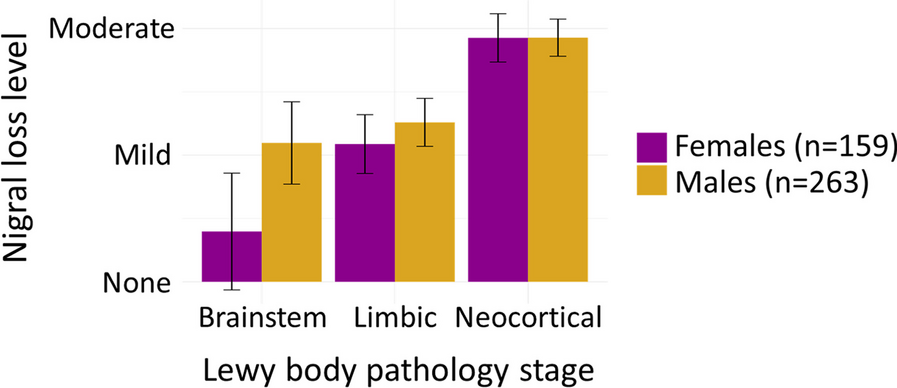
We included 159 females and 263 males with brainstem, limbic, or neocortical Lewy body pathology from the National Alzheimer’s Coordinating Center database. We identified whether people had clinician report of Lewy body dementia core features (cognitive fluctuations, visual hallucinations, rapid eye movement sleep behavior disorder, parkinsonism) during follow-up. We used generalized linear models adjusting for age and Alzheimer’s pathology staging for the association between nigral loss and (1) Lewy body pathology staging, (2) presence of Lewy body dementia core features. We also assessed whether any of the core clinical features can predict underlying nigral loss using the clinical profile at the first visit with dementia.
Similar to our previous papers, we noted that females died older and had higher levels of Braak tau staging. However, Lewy body pathology staging and nigral loss levels were similar for females and males. Females were less likely than males to have a Lewy body dementia phenotype. We found that more advanced Lewy body pathology staging was associated with more severe nigral loss, more so for males. In terms of nigral loss association with clinical features, more nigral loss was associated with a higher likelihood of parkinsonism and Lewy body dementia phenotype, more so for males. We did not identify any core features associated with nigral loss at the first visit with dementia in a subgroup of 40 females and 58 males who developed dementia during follow-up.
These findings build up on our previous reports in the National Alzheimer’s Coordinating Center data for people with pathologically-defined Lewy body dementia. Similar to Lewy body and Alzheimer’s pathology correlates differing by sex, nigral loss correlates also differ by sex. Females with Lewy body pathology have a higher risk of underdiagnosis compared to males, even when they have lower levels of Alzheimer’s pathology and higher levels for nigral loss. Furthermore, as we utilize DaTScan, which correlates with nigral loss, as a supportive biomarker for Lewy body dementia, the utility of this biomarker likely differs by sex. Understanding why females may not develop dementia or other symptoms despite having as much pathology as males, can help with therapeutic efforts.
Follow the Topic
-
Biology of Sex Differences
This journal is unlike any other scientific journal: articles focus on sex differences in all aspects of an individual or organism. Everything from molecules to behavior and from studies of cellular function to clinical research studies are reported in this journal.

Related Collections
With Collections, you can get published faster and increase your visibility.
Sex Differences in Metabolic Regulation and End-Organ Damage
Sex differences profoundly influence endocrine and metabolic regulation, shaping disease susceptibility, progression, and therapeutic responses. This Collection aims to highlight how hormonal and metabolic interactions contribute to sex-specific pathophysiology across a range of endocrine disorders and associated systemic complications.
Research topics of interest include mechanisms and therapies addressing hormonal and metabolic dysregulation observed in conditions such as polycystic ovary syndrome (PCOS), metabolic syndrome, diabetic nephropathy, thyroid disorders, Cushing’s syndrome, and hyperaldosteronism. Emphasis is also placed on how these disorders impact multiple organ systems including the cardiovascular and renal systems, resulting in sex-specific patterns of end-organ injury and disease progression. Original research, clinical trials, translational studies, and comprehensive reviews are welcome.
Subtopics include, but are not limited to:
- Hormonal regulation of glucose and lipid metabolism by estrogens, androgens, and progesterone
- Sex-specific metabolic adaptations in obesity, diabetes, and cardiovascular disease
- Neuroendocrine and inflammatory mechanisms linking hormones to metabolic dysregulation
- Cardiovascular and renal complications of endocrine dysfunction
- Neuroendocrine control of metabolic homeostasis
- Endocrine disorders with metabolic manifestations
- Sex-based differences in drug response and therapeutic outcomes
All submissions in this Collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Nov 04, 2026
Sex Differences in Cardiovascular Disease
Sex differences play a crucial role in the development, presentation, and treatment of cardiovascular disease. Despite growing recognition of these differences, major gaps remain—particularly in understanding how biological sex and gender influence risk, diagnostics, disease mechanisms, and therapeutic outcomes. This Collection aims to address these gaps by bringing together high-quality research that advances sex-specific and gender-aware cardiovascular science.
Key areas of interest include the impact of hormonal transitions such as menopause, pregnancy-associated cardiovascular conditions, and the distinct mechanisms underlying female-predominant conditions such as HFpEF and microvascular dysfunction. Understanding these processes is essential for developing accurate risk prediction models and personalised treatment strategies.
Persistent gender disparities in diagnosis, management, and access to care also contribute to poorer outcomes—issues that remain central to achieving equitable cardiovascular health. By encouraging research across these domains, this Collection aims to support scientific progress and clinical innovation that benefit individuals of all sexes.
Possible topics include but are not limited to:
- Menopause and cardiovascular risk
- Pregnancy-associated cardiovascular disease
- Sex differences in heart failure with preserved ejection fraction (HFpEF)
- Sex differences in arrhythmias
- Microvascular dysfunction in women
- Sex-specific platelet reactivity
- Gender disparities in cardiovascular treatment
- Sex-specific cardiovascular risk prediction models
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this Collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 16, 2027
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in