SPECTRUM OF BRAF MUTATIONS IN PAKISTANI COHORT
Published in Cancer and Biomedical Research
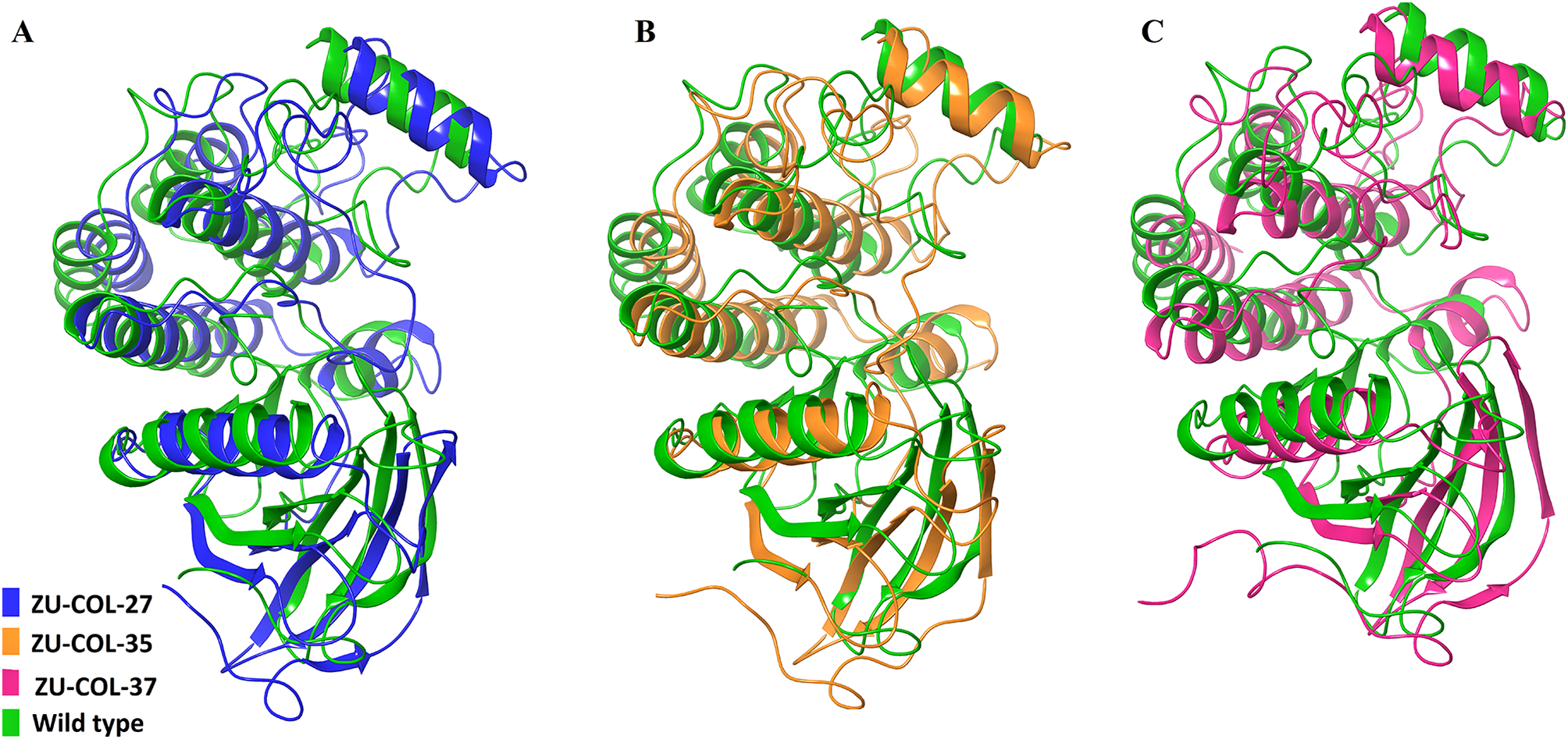

Colorectal cancer remains a major cause of cancer-related morbidity and mortality worldwide, yet genomic profiling and personalized oncology are far from being a clinical reality in many underdeveloped countries. Our motivation stemmed from a deep concern over this disparity. Despite a growing burden of colorectal cancer in our region, there was a notable absence of local molecular data, particularly regarding actionable mutations such as KRAS and BRAF, which guide prognosis and therapy.
We aimed to generate baseline genomic data regarding BRAF mutations for our local population and identify associated molecular events. Genetic testing services in our country are accessible only to a privileged few, and targeted therapy options are virtually non-existent in public-sector hospitals. This reality adds urgency to our efforts, as the lack of infrastructure perpetuates a cycle of late diagnosis, suboptimal treatment, and poor outcomes.
We hope our work not only contributes to colorectal cancer research but also highlights the need for greater investment in molecular oncology infrastructure in under-resourced settings.
Follow the Topic
-
BMC Cancer
This is an open access, peer-reviewed journal that considers articles on all aspects of cancer research, including the pathophysiology, prevention, diagnosis and treatment of cancers.

Related Collections
With Collections, you can get published faster and increase your visibility.
Prehabilitation in cancer
Prehabilitation in cancer care is an emerging field focused on optimizing patients' physical and psychological well-being prior to undergoing surgery or treatment. By incorporating strategies such as exercise, nutritional support, and psychological interventions, prehabilitation aims to enhance patients’ resilience and overall health outcomes. The concept has gained traction as healthcare professionals recognize the significance of preparing patients for the demands of cancer treatment and recovery, ultimately aiming to improve surgical outcomes and quality of life.
The importance of integrating prehabilitation into cancer care has been underscored by recent advances in research demonstrating its potential benefits. Studies have shown that tailored exercise programs and nutritional interventions can significantly improve treatment outcomes, reduce complications, and enhance recovery times. As healthcare systems increasingly prioritize patient-centered approaches, the implementation of prehabilitation practices may lead to more effective cancer management and improve the overall experience for patients navigating their cancer journey.
Continued research in this area has the potential to revolutionize cancer care practices, paving the way for the development of standardized prehabilitation protocols tailored to individual patient needs. This research may also inspire innovations in telehealth and digital health solutions that facilitate remote prehabilitation interventions, making these essential services more accessible to patients regardless of their geographical location.
Topics welcome to this Collection include, but are not limited to, the following:
- Impact of prehabilitation on surgical outcomes
- Exercise interventions in cancer care
- Nutritional support during prehabilitation
- Prehabilitation and chemotherapy outcomes
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 20, 2027
Cancer control in low- and middle-income countries – Part II
In recent years, non-communicable diseases, including cancer, have shown a disproportionate increase in incidence and related mortality in low- and middle-income countries (LMICs). By 2030, approximately three-quarters of all cancer deaths will occur in LMICs, with one in eight people experiencing a cancer diagnosis in their lifetime. Reasons for disparate trends include better risk factor control in high-income countries (lower infection-associated cancers, anti-smoking campaigns, and other preventive measures), educational resources, increased number of screening and surveillance programs with earlier detection of disease, and access to more effective cancer therapies. In contrast, many LMICs experience rising cancer incidence rates due to demographic transitions marked by aging population structures and a shift in prevalent risk factors (e.g., increasing tobacco use, alcohol consumption, unhealthy diets, physical inactivity). The underlying factors are complex and interrelated, contextualized to each country's setting, and merit further study.
In 2015, the United National General Assembly adopted the 2030 Agenda for Sustainable Development Goals (SDGs), built on the principle of “leaving no one behind.” The goals highlighted the importance of fighting inequalities across the world, and specifically, two goals, SDG 3: Good Health and Well-Being and SDG 10: Reduced Inequalities, have the ambitious aim of reducing disparities within and among countries and ensuring healthy lives for all at all ages. In addition, the 2020 WHO report on cancer clearly states that cancer control is an integral component of the path toward universal health coverage and achieving SDGs. By investing wisely and equitably, cancer cases and deaths can be avoided, and premature mortality can be reduced by 2030.
Hence, to combat the high mortality of preventable and treatable cancer in LMICs, urgent efforts are needed to improve cancer control programs and educate the public to bridge knowledge gaps, address misconceptions, and debunk myths. In addition, several gaps in the research enterprise of LMICs, such as the scarcity of reliable data, a lack of clinical trials, as well as the lack of infrastructure and trained human resources, must be addressed to solve local and regional problems with acceptable, feasible, effective, and implementable solutions.
In recognition of this relevant field, we encourage submissions including but not limited to those addressing:
• Patient navigation in cancer care and its role in cancer control in LMICs
• Training of the workforce caring for patients with cancer in LMICs
• Decentralization of cancer care in LMICs
• Technology, infrastructures, and the need for implementation in cancer care in LMICs
• The role of AI and digital health in cancer care in LMICs
• Financial burden of cancer care on patients and their families
• The role of cancer registries in strengthening cancer control in LMICs
• Defining optimal cancer treatment approaches in LMICs using local evidence
• Clinical trials and cancer in LMICs
• Anticipation medicine and cancer in LMICs
• Trends in cancer research in LMICs
• National cancer control plans and their utility in LMICs and barriers to implementation
• Twinning and partnership in cancer care in LMICs
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer-review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 3: Good Health and Well-Being and SDG 10: Reduced Inequalities.
Publishing Model: Open Access
Deadline: Aug 14, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in