The Doorbell Rang at 10:53
Published in Healthcare & Nursing, Research Data, and Biomedical Research

Beginning Breaks & Bruises
The doorbell rang at 10:53; a Global Burden of Disease Study lead epidemiologist was calling at 11:00. I’d sought his expertise on how to estimate the disability weight of Long COVID, so I could calculate its ‘years lived with disability (YLD).’ In my haste to finish with the visitor outside so I’d be at my desk at 11:00, I raced down our concrete steps and fractured three toes — giving me a small, temporary, and self-inflicted taste of what ‘years lived with disability’ feels like. Dragged inside by my younger daughter, laptop propped on the couch where I lay, my first words to Dr. Theo Vos were: ‘I think I’m going to pass out. Can we reschedule?’
Close to Home: Personal and Professional
This was June 2023 — more than three years after the March 2020 lockdowns. Research until then centered on acute COVID morbidity and mortality, not its potent sequelae. As Dr. Anthony Fauci remarked in a Fall 2022 interview: ‘It’s a very insidious, beneath-the-radar-screen public health emergency…. [F]unction is being considerably impaired…[but] that doesn’t attract as much attention as a death rate.’ By then, disability accounted for most Long COVID disease burden; women bore its brunt. There were no treatments or active trials to find one, nor data on Long COVID’s disability burden and relative research funding in the US.
This research has been a labor of love. My now early-30s older daughter lost her senses of smell and taste in March 2020. Though never hospitalized, her Long COVID symptoms included GI, chest and muscle pain, and depression secondary to Long COVID. The vibrant young woman who loved tennis and hiking couldn’t walk two blocks without spiking her heart rate. Being diagnosed with postural orthostatic tachycardia syndrome (POTS) — a nervous system disorder often triggered by viral infection — was a ‘validation’ of sorts. At the time, Long COVID — like ME/CFS, fibromyalgia, migraine, and Lyme disease — was a ‘contested illness’: medically unexplained symptoms that predominantly affect females who have struggled to get medical professionals to believe their complaints.
My research focuses on disability. I co-direct our University Center for Excellence in Developmental Disabilities (UCEDD) Research and Service. From 2021–2023 I led a grant to equip New York State’s disability community with science-based information about COVID vaccines. Watching my daughter’s treatment dead-ends — and providers who often knew less than her (she has an MPH) — activated my UCEDD brain. Like Long COVID, developmental disabilities (e.g., autism, intellectual disability) are “non-visible,” as are ≈75% of disabilities. Beyond that, I’d never conducted research on either infectious disease or disease burden — though years of teaching epidemiology to first year medical students proved more useful than I expected.
Disability Data Dilemmas
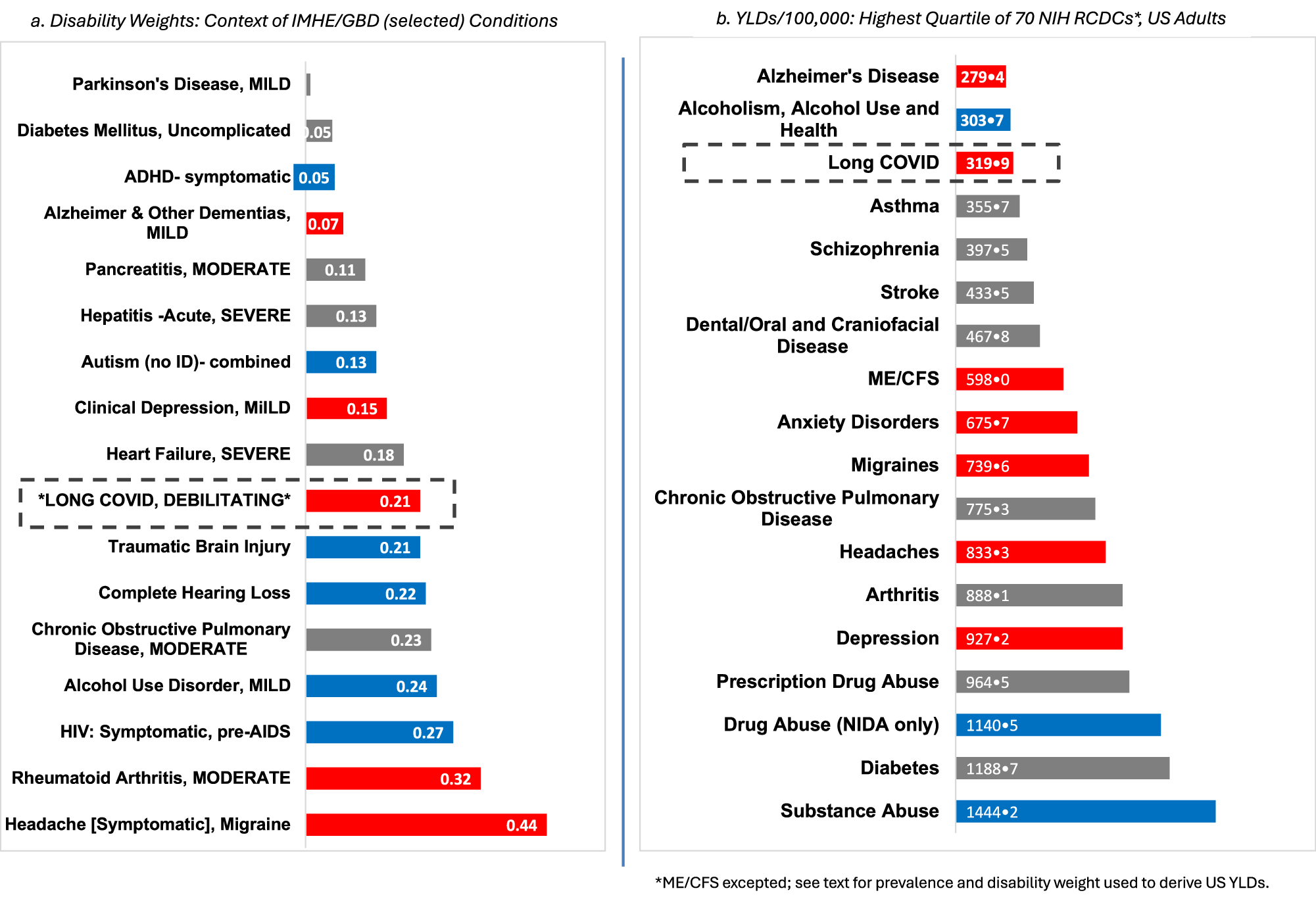
To contextualize Long COVID’s disease burden relative to other conditions and their research funding — I first had to settle on a disease burden metric. I chose YLDs over the more commonly used ‘disability adjusted life years (DALYs)’ or ‘years of life lost to disease (YLLs).’ I did so because 1) disability — not death — accounted for most COVID burden by 2023, 2) YLDs are better measures of burden for chronic conditions, which Long COVID had become and 3) there weren’t the longitudinal data needed to estimate YLLs. YLD is calculated as: YLD = prevalence × disability weight.
After selecting a disease burden metric for Long COVID, work turned to finding data sources, operationalizing terms, and harmonizing data sets, i.e.:
- Sourcing data on Long COVID prevalence in the US, and how to operationalize disabling Long COVID in those data
- Mapping conditions/categories between the NIH “Research, Conditions and Disease Categories (RCDC)” and the Global Burden of Disease Study- to pinpoint funding for US-based YLDs
- Quantifying Long COVID funding- outside of the NIH RCDCX website
So, What Did We Find?
Long COVID ranked in the top quartile of disability burden across all 68 conditions — yet received just 14% of the NIH funding its burden warrants ($106M vs. $739.8M; FY2022-2024 annual average). Conditions predominantly affecting women received 5.2 times less funding per YLD than those predominantly affecting men. ME/CFS, which frequently co-occurs with Long COVID, fared worst of all — receiving less than 1% of its commensurate funding. The data make a simple point: what disables people should be more of a driver of what we fund.
Living Life- Changed by Long COVID
As for my older daughter? She has been able to work with ADA accommodations, living her life at a slower pace than she might have anticipated. And even several years later, I can predict a storm by the pain in my right foot. The research is moving- but not fast enough for the millions who remain sidelined by Long COVID.

I enjoy walking by an area reservoir, yoga, and cooking and baking vegetarian and no refined sugar (respectively!) dishes. I am also active in local civic engagement and spiritual communities.
I am a Professor in the Department of Family and Social Medicine at Einstein College of Medicine-Montefiore Medical Center (Bronx, NY), where I co-direct our University of Center of Excellence in Developmental Disabilities (UCEDD).
I became interested in the impact of Long COVID after my previously healthy daughter in her late 20s was impacted by it. This study drew on buth my training in epidemiology and research, and my UCEDD role in conducting disability research.
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Exercise and Physical Activity in Health and Disease
Publishing Model: Open Access
Deadline: Sep 03, 2026
Life Course Epidemiology
Publishing Model: Open Access
Deadline: Sep 30, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in