Very old patients need palliative care,not intensive care - an empirical and normative analysis
Published in Mechanical Engineering and Philosophy & Religion
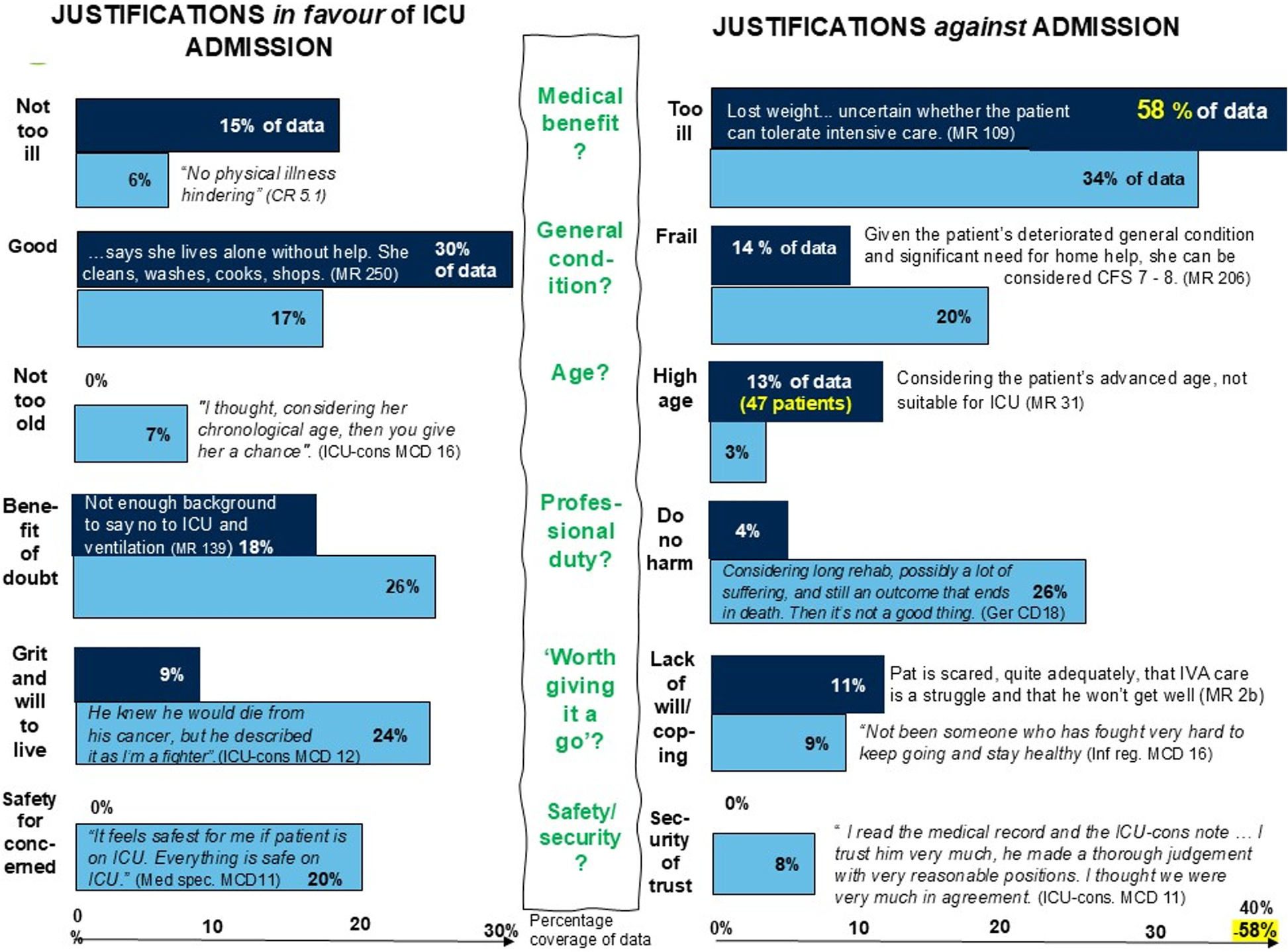

We found clear and consistent evidence – both quantitative and qualitative – that high chronological age is a key factor against ICU admission. Among all the variables we compared, only being 80 years or older clearly stood out as linked to not being admitted to intensive care.
Across every data source, high age kept reappearing as a justification for non-admission. In medical records, “considering age” was mentioned again and again. In the COVID Rounds, Moral Case Deliberations (structured reflections on ethically complex patient cases), and follow-up interviews, the phrase “very old” was used repeatedly when decisions were discussed.
Another powerful justification across all data was about not harming the patient. This included avoiding unworthy suffering, not subjecting patients to what was described as torture when ICU care offered no benefit and recognising ventilator treatment as risky. For patients over 80, ICU care was often described as unacceptable; at 90, death was seen as a natural event. One ICU consultant put it poignantly:
“Ninety feels like, if you’ve had a good life and you’re spry and healthy ... if you die suddenly, then it’s expected. And better than dragging to the ICU and tormenting the person.”
Interestingly, few justifications were directly linked to the pandemic. The patterns we found mirror those from pre-COVID studies, suggesting that what we captured ordinary clinical decision-making, not crisis-specific thinking.
Normative discussion
When discussing chronological age as a factor, our findings align with two key ethical principles: non-maleficence and justice.
Non-maleficence implies here sparing patients from unnecessary suffering and loss of dignity. Distributive justice connects with the ICU prioritisation literature, which tends to exclude patients “with a fuller lifecycle.” In intensive care, defining what counts as a need becomes crucial.
According to Swedish legislation, healthcare needs are defined by both the severity of a condition and the potential benefit of treatment. For very old patients, with higher ICU mortality and poorer recovery rates, the potential benefit is often limited. From this perspective, ICU care may not truly meet very old patients’ needs.
Following the legal principle of Need and Solidarity, treatment should only be prioritised when there is potential for benefit. Our results therefore suggest that many very old patients are better served by palliative rather than intensive care.
A call for courage and clarity
We believe it is time for a national – and perhaps international – guiding policy on triage systems for very old patients in everyday care. Such a policy should be developed with courage and transparency, openly supporting a palliative approach for the very old.
Follow the Topic
-
BMC Medical Ethics
This journal is an open access journal publishing original peer-reviewed research articles in relation to the ethical aspects of biomedical research and clinical practice, including professional choices and conduct, medical technologies, healthcare systems and health policies.

Related Collections
With Collections, you can get published faster and increase your visibility.
Ethical challenges in outbreak response
BMC Medical Ethics is calling for submissions to our Collection, Ethical challenges in outbreak response. The emergence of infectious disease outbreaks presents numerous ethical challenges that require careful consideration by public health officials, healthcare providers, and policymakers. As outbreaks escalate, the need for rapid decision-making often clashes with the principles and values that underpin clinical and public health ethics. This Collection aims to explore these dilemmas, focusing on the intersection of ethics and crisis management during outbreak response. We welcome work that critically reassesses governance failures during the COVID-19 pandemic, other outbreaks, and/or anticipates "Disease X" scenarios. The collection seeks to provide a platform for discussing normative tensions distinctive to outbreak contexts, such as urgency, uncertainty, collective risks, and coercive powers.
Addressing ethical challenges in outbreak response is crucial for ensuring that future public health interventions are fit for purpose. In addition to substantive principles, there is now increased attention to the procedural justice that should guide public health decisions in crises, emphasizing the need for transparent, inclusive, and participatory approaches. As societies grapple with the complexities of managing outbreaks, examining these ethical dimensions will be vital for fostering public confidence and ensuring the effectiveness of interventions in future outbreaks.
This Collection welcomes critical reflection on the strengths and limits of existing ethical frameworks for outbreak response, including their capacity to address contextual complexity, power asymmetries, and global inequities.
Topics of interest include but are not limited to:
- Ethical dilemmas in resource allocation
- Tensions between individual rights and coercion for collective ends
- Consent and authorization in conditions of urgency, uncertainty, and constrained liberty
- Public trust in health systems
- Crisis management ethics
- Reciprocity and occupational risk (healthcare workers, essential workers)
- Global justice and structural inequalities
- Bioethical frameworks for outbreak response
- Ethics in pandemic preparedness
We welcome normative, empirical, and interdisciplinary contributions that critically examine how ethical commitments are negotiated, operationalized, or compromised in outbreak response.
Researchers are invited to submit their work to this Collection, showcasing insights into the ethical challenges faced during outbreak response and exploring innovative solutions to ensure ethical practices in public health.
This Collection supports and amplifies research related to SDG 3 (Good Health and Well Being) and SDG 10 (Reduced inequalities).
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer-review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Dec 11, 2026
Digital determinants and ethical AI in global health
BMC Medical Ethics invites submissions to our new Collection, Digital determinants and ethical AI in global health. The integration of digital technologies and artificial intelligence (AI) into healthcare has transformed the landscape of global health, introducing new opportunities and challenges. As these technologies become more embedded in clinical practice and public health strategies, emphasizing the ethical implications surrounding their use is crucial.
Recent advancements have highlighted the necessity for algorithmic transparency and accountability, as well as the need for inclusive approaches to AI that prioritize health equity. With this, researchers are encouraged to contribute to a more equitable healthcare system that respects patient rights and fosters trust in digital health solutions. Embedding ethical considerations at the forefront of digital innovation, rather than treating them as secondary concerns, is critical to ensuring that emerging technologies do not reinforce existing health inequities.
This Collection examines the intersection of digital determinants and ethical AI, with particular attention to informed consent, algorithmic transparency, and the implications of emerging technologies for patient autonomy and healthcare equity. To ensure a genuinely interdisciplinary dialogue, we invite submissions from physicians, legal scholars, philosophers, engineers, computer scientists, data scientists, and other digital‑technology professionals. Key areas of interest include, but are not limited to:
- Informed consent in digital health
- Algorithmic transparency and accountability
- Equity and inclusion in AI healthcare solutions
- Bias in AI diagnostics and decision-making
- Ethical implications of data privacy in digital health
- The interaction between digital determinants and other determinants of health
- Digital literacy in global health projects
- The impact of large language models (LLMs) on global health and their role as digital determinants of health
- Emerging debates about AI in One Digital Health
- Ethical discussions on the sustainability of AI and the environmental effects of health digitalization at a global scale
- Comparative analyses of data governance models, AI, and other digital technologies in relation to their impacts on global health
This Collection supports and amplifies research related to SDG 3: Good Health and Well-Being.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer-review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 13, 2027



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in