Why and How Health Research Must Escape Linear Thinking
Published in Social Sciences, Computational Sciences, and Public Health

A podcast version of this article is available for those who prefer to tune in: Listen here.
The claim: linear thinking can reproduce inequity
Health research has a public health problem that goes beyond methodology. It is not only that we sometimes choose the wrong study design, outcome measure, or implementation framework, but also that we often use a linear imagination to study systems that are not linear.
That matters because linear thinking is not neutral. When policy assumes that access is simple, when services assume that care begins at referral, when implementation assumes that evidence travels cleanly from trial to practice, and when digital health assumes that technical performance is the same as real-world benefit, the result can be exclusion. The people most affected are often those public health is meant to protect: homebound people, First Nations Peoples, rural and remote communities, older adults with multimorbidity, people navigating fragmented chronic care, and patients expected to trust unfamiliar technologies.
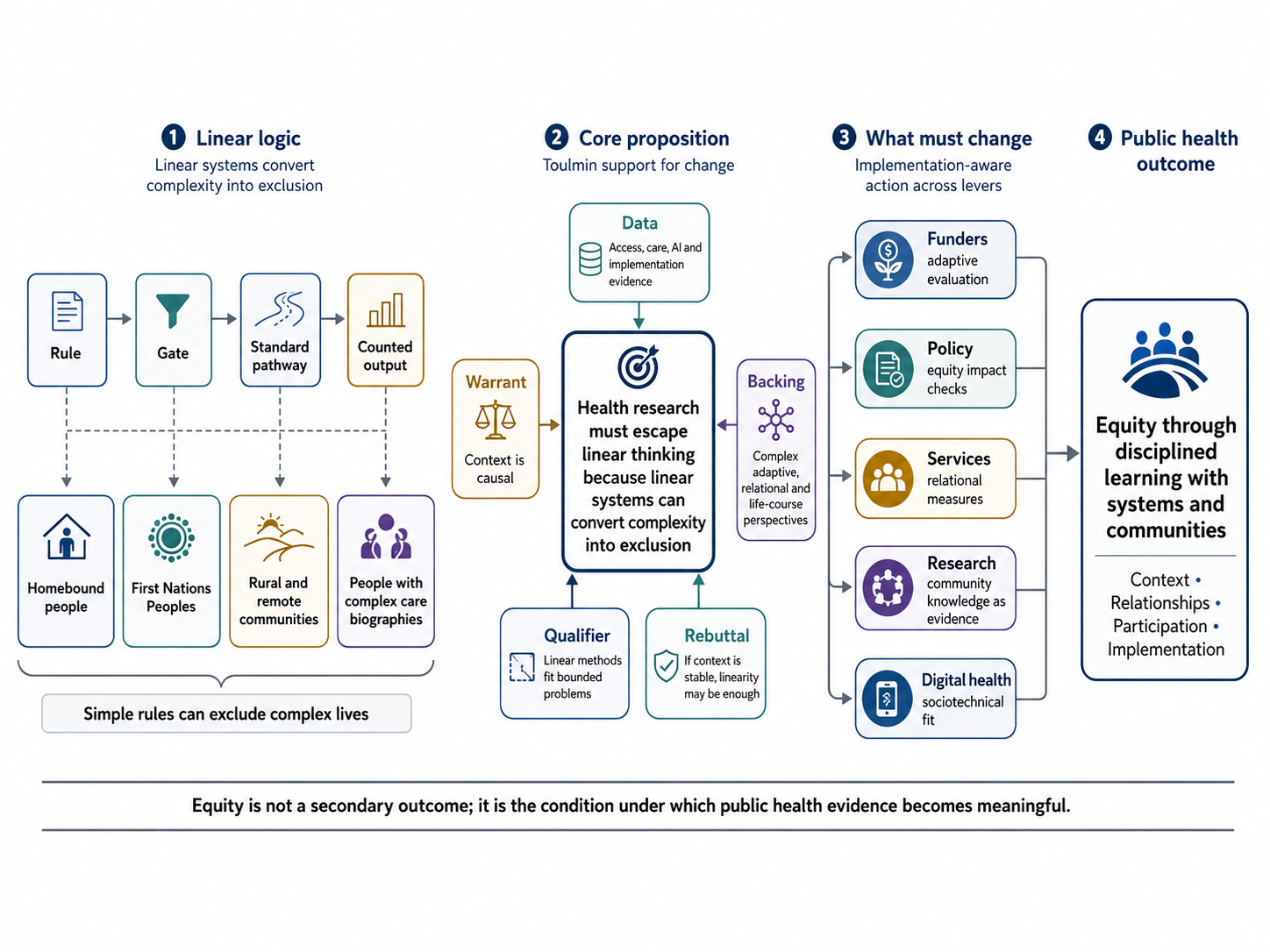
The central claim of this article is therefore simple: health research must escape linear thinking because linear systems often convert complexity into exclusion.
This is not a rejection of rigour. It is a rejection of the wrong kind of rigour for the wrong kind of problem. Linear methods have value when questions are bounded, causal pathways are clear, and contexts are stable. Randomised trials, predefined protocols and project management can be essential in those circumstances. However, many urgent public health problems are not like that. Chronic disease, health inequity, ageing, workforce pressure, digital transformation and clinical artificial intelligence are wicked problems shaped by contested evidence, values and power [1]. They change as we act on them, involve multiple actors, and expose disagreement about whose knowledge counts.
The warrant for the argument is that a method is rigorous only if it fits the problem. When the problem is complex, adaptive, relational and political, rigour must include context, relationships, lived experience, uncertainty, implementation conditions and unintended consequences.

The data: access rules reveal the failure
The clearest evidence comes from access. During the COVID-19 pandemic, temporary telehealth initiatives changed what care could mean for many Australians. Frail, homebound and bedridden people could receive care without the physical burden of attending appointments. This raised a basic public health question: if a person is not well enough to attend an appointment, should the system interpret that as non-attendance or as evidence that the access model is failing them? [2]
When telehealth funding rules changed, Medicare access for many patients became tied to an existing clinical relationship or a face-to-face visit at the practice within the previous 12 months, although exemptions apply [3]. From a linear administrative perspective, this rule may appear reasonable, because it seeks to protect continuity, safety and appropriate use. From a public health systems perspective, the same rule reveals a contradiction: a policy designed to regulate access may unintentionally exclude people with the greatest need for access.
This is an argument from consequences. If the consequence of an access rule is that homebound people are less able to use a service designed to improve access, then the rule must be evaluated not only for administrative coherence, but for equity. A policy can be internally logical and publicly harmful at the same time.
This program of work has contributed to Australian policy discussion through evidence on telehealth access as a structural equity issue [4], national chronic disease reform focused on equity, integrated care and priority populations [5], and integrated services for chronic disease and social and emotional wellbeing [6]. It has also contributed to the translation of flexible, person-centred cardiac rehabilitation into South Australia’s statewide cardiac rehabilitation model of care [7].
The point is not that telehealth is automatically equitable. It is not. The point is that a technology designed for access can become inequitable when policy logic does not account for embodiment, geography, disability, trust, continuity and practical ability to attend. A linear model asks whether telehealth works. A public health systems model asks who it works for, under what rules, through which relationships, with what barriers, and with what unintended consequences.
The warrant: participation is evidence, not decoration
If systems fail because they cannot see the realities they affect, then consumer and community knowledge is not a decorative addition to research. It is part of the evidence base.
A large systematic review and meta-analysis of consumer engagement examined 23 randomised controlled trials involving more than 136,000 participants [8]. Most engagement strategies were consultative and concentrated in the development phase. The strongest evidence of impact came from large cluster-randomised trials in community-based maternal health services, where higher levels of public participation were associated with significant reductions in neonatal mortality [8].
The inference here is not that every project requires the same form of participation. That would simply replace one rigid formula with another. The stronger inference is that participation must be proportionate to the problem. If the problem involves lived experience, access, trust, cultural safety, marginalisation or service fit, then consultation alone is unlikely to be enough. People affected by the system must help define the problem, interpret the evidence, design the response and judge whether the outcome matters.
This is an argument from epistemic authority. Consumers, carers, clinicians and communities know things that researchers and policymakers cannot know from administrative data alone. They know how care feels when it is fragmented, how services fail when transport is impossible, how distrust accumulates, how family obligations shape adherence, and how dignity can be lost in systems that appear efficient on paper. To ignore this knowledge is not only ethically weak; it weakens the science.
The analysis of wicked problems and knowledge translation makes the political dimension clearer [1]. Knowledge translation is not merely a technical process of moving evidence into practice. It is also a political process concerned with whose knowledge is recognised, whose expertise is protected and whose realities are allowed to shape decisions. In an era where expertise is contested and alternative facts proliferate, democratising knowledge is not a threat to rigour; it is one of the ways rigour is defended.
For public health, this matters because inequity is not produced only by a lack of services. It is also produced by a lack of interpretive power. When communities are asked to comment on systems they did not help design, when lived experience is collected but not allowed to change the decision, and when marginalised populations are consulted only after the policy pathway is already fixed, participation becomes symbolic rather than transformative.
The backing: research governance must learn, not only control
If the warrant is that complex problems require methods that can see context, then research governance must also change. Project management is useful for coordination, but it becomes a constraint when mistaken for the logic of inquiry itself.
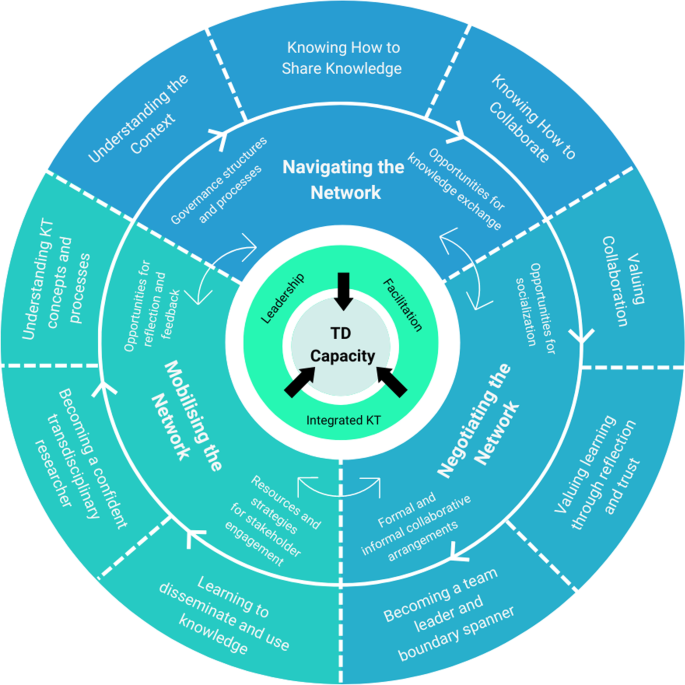
A realist evaluation of transdisciplinary research and knowledge translation examined how a five-year NHMRC-funded Centre of Research Excellence learned to work across disciplinary and practical boundaries [9]. The important finding was reciprocal: transdisciplinary research and knowledge translation shape each other. Teams do not simply produce evidence first and translate it later; they learn to translate knowledge as they learn to work together.
This is an argument from causal mechanism. Complex health research becomes useful not only because it produces outputs but also because it builds relationships, shared language, trust, facilitation, and distributed leadership through which knowledge can move. Those mechanisms are not secondary to the research; they are part of how impact becomes possible [9].
The methodological backing for this position is PROLIFERATE, which treats context, feedback, and adaptation as evidence [10]. PROLIFERATE does not treat emergence, feedback loops and contextual variation as contamination. It treats them as data. It asks researchers to examine how innovations interact with systems, how systems respond, and how learning can be used to optimise implementation over time.
The same argument appears in the call to free transdisciplinarity from the project straightjacket [11]. Transdisciplinarity seeks to address problems that cannot be fully predefined, whereas conventional project management assumes that the problem can be bounded in advance. The mismatch is structural, not incidental.
This is where the qualifier matters. If a health problem is stable, the intervention is well-defined, and the implementation environment is predictable, conventional project governance may be sufficient. If the problem is emergent, contested and distributed across actors and settings, rigid project logic can inhibit the very learning it claims to organise. A public health research system, therefore, needs more than accountability for outputs. It needs accountability to learning, adaptation, equity, relationships and emergent outcomes. Milestones matter, although they cannot be the only proof that research is working.
The deeper structure: care does not begin at referral
The argument becomes stronger when it moves from access to care itself. Health systems often treat care as a set of tasks delivered during clinical episodes. Patients experience care differently, as a life course: a sequence of encounters, relationships, ruptures, recoveries, disappointments, adaptations and memories.
This difference is visible in cardiac rehabilitation. A population-level analysis of cardiac rehabilitation access and completion found that only 31.9% of 84,064 eligible discharged patients in South Australia were referred. Of those referred, 36.8% commenced, and 77.8% of those who commenced completed [14]. Female sex, depression and waiting times over 28 days predicted non-completion. Telehealth enrolment was associated with lower odds of completion, a finding that warrants careful interpretation, as telehealth was often used as a fallback option for people already facing barriers, rather than being designed as a first-choice pathway for those who were homebound or geographically isolated.
These numbers are important, although numbers alone cannot explain disengagement. A person does not enter cardiac rehabilitation as a blank clinical subject. They bring previous care experiences, social conditions, family responsibilities, cultural expectations, fear, trust and sometimes exhaustion.
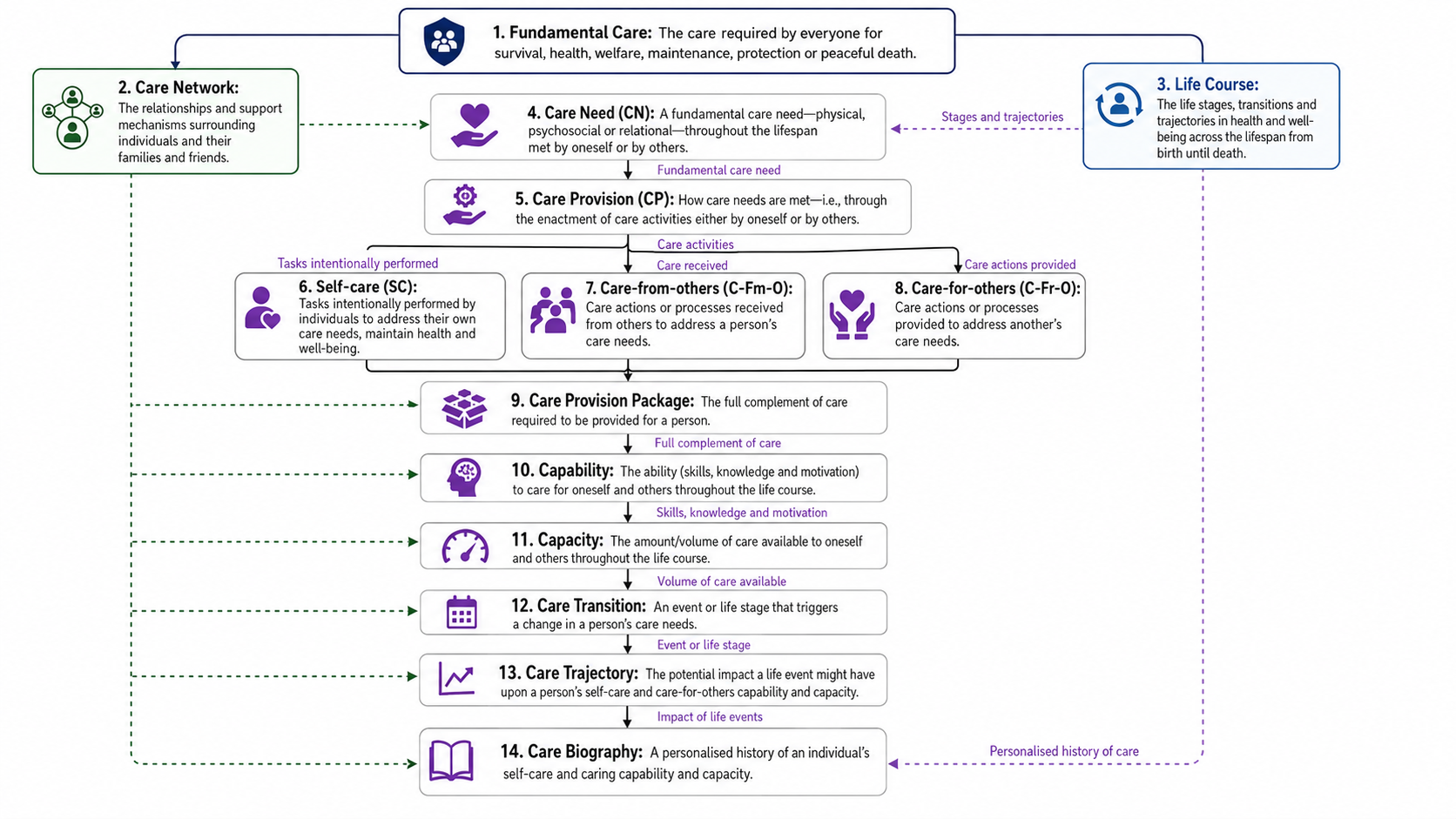
This is where care biography, as accumulated care experience, becomes essential [15]. Care biography refers to the accumulated narrative of a person’s care experiences over time, shaped by relationships, contexts and transitions. It helps explain why someone who has experienced fragmented, unsafe, disrespectful or culturally inappropriate care may resist or disengage from a program that appears clinically appropriate, yet is biographically misaligned.
The Caring Life Course Theory extends this argument by showing why care must be understood across biographies, networks, transitions and relational contexts [16]. Applied to cardiac rehabilitation, this shows that care from others, capability, care networks, and care provision are interconnected, while gaps between care biography, fundamental care, and self-care reveal why services may remain incomplete even when technically available [16].
This is an argument from sign and explanation: Disengagement is not simply a sign of individual non-compliance. It may be a sign that the service model does not fit the person’s biography, relationships, context or trust history. The explanation is not always inside the patient. It is often in the relationship between the patient and the system.
The same logic appears across populations. In self-care among older adults with multimorbidity, self-care was not a solitary behaviour; it was a socially embedded practice shaped by care networks, life transitions and accumulated care experiences [17]. In prostate cancer survivorship, care biographies shaped how men interpreted care needs, care trajectories and self-care behaviours before and after treatment [18]. A review of self-management support for socioeconomically disadvantaged older adults confirmed that effective interventions are not simply those with sophisticated protocols, but those that build on strengths, respect social circumstances and provide flexible, person-centred support [19]. The conclusion is difficult and necessary: health systems cannot improve engagement by treating patients as if they begin at the point of referral. They begin much earlier, in the accumulated history of care.
Cultural continuity is not an implementation detail
The argument from care biography becomes a public health equity argument when applied to First Nations continuity of care. The issue is not simply whether services exist. The issue is whether care is continuous, culturally responsive, relationally safe and meaningful across the life course.
Evidence on continuity of care for First Nations Peoples living with chronic disease identified barriers such as inadequate community initiatives, weak health and social care networks, and insufficient coaching and peer support [13]. The enablers were relational and cultural: care adapted to cultural beliefs, family influences, and lived realities; continuing and trusting relationships among providers, patients, and caregivers; and flexible, consistent, and adaptable care across the continuum [13].
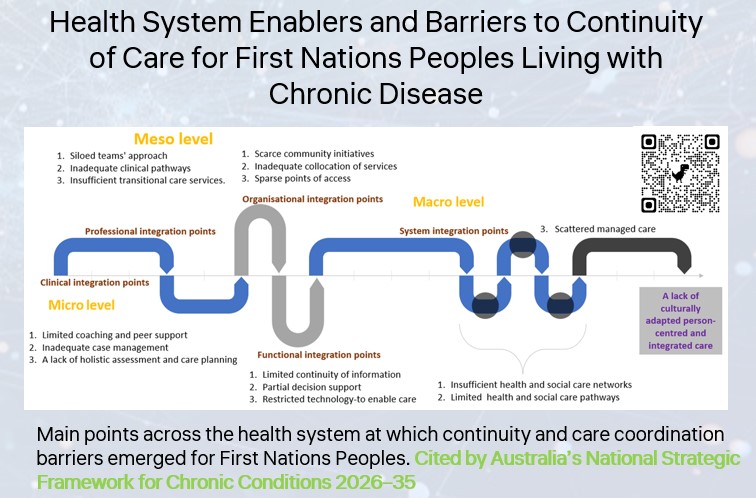
This is an argument from values and practical reasoning. If public health values equity, self-determination, and culturally safe care, then continuity cannot be reduced to service contact alone. A person can attend appointments and still experience care as fragmented, unsafe or culturally misaligned. Care becomes continuous when relationships, meanings, family contexts and community priorities are recognised as part of the system.
The policy relevance of this evidence is visible beyond academic publication. It has been taken up in national policy spaces concerned with continuity of care, health equity, integrated care and culturally responsive chronic disease management [5], and in an AIHW report where integrated services, trust, care coordination, multidisciplinary care and system-level supports are treated as necessary conditions for better chronic disease care and social and emotional wellbeing for First Nations people [6].
Public health cannot treat culture as an implementation detail after the evidence is produced. Culture shapes whether care is trusted, whether services are navigable, whether continuity is meaningful, and whether health systems are experienced as safe. In that sense, cultural continuity is not separate from effectiveness; it is one of the mechanisms through which effectiveness becomes possible.
Technology is a sociotechnical intervention, not a neutral tool
The same reasoning applies to digital health and AI. Health systems often treat technology as if implementation follows naturally from technical performance. In practice, a tool can be accurate and still fail if it cannot be understood, trusted, integrated into workflow or used equitably across different levels of experience and resourcing.
The review of telehealth as a care solution for homebound people found that telehealth can reduce healthcare utilisation and improve health-related quality of life and wellbeing for homebound populations [20]. The policy question remains, however: if access depends on recent in-person attendance for many patients, then the intervention may be least available to those who most need it [3]. This is a classic systems contradiction. Evidence shows potential benefit, while policy design can constrain real-world equity.
Measurement work makes the same point from the care side. The relationship between care context, therapeutic relationship and integrated care was validated in a Spanish-speaking hospital population of 1,053 patients [21]. The patient-centred measurement of caring interaction then extended this agenda by modelling caring interaction from the patient’s perspective [22]. Together, these tools make a strong claim: relational care is not too soft to measure, it is too important not to measure.
The same principle applies to AI. Systems-aware evaluation of clinical AI led to the adoption of PROLIFERATE_AI in cardiac care [23]. It was then applied to human-centred AI for emergency cardiac care, where evaluation considered not only technical performance, but also comprehension, usability, clinician trust, workflow integration and contextual variation [24].
This is an argument from practical consequences and risk: A technically accurate AI tool may still widen inequities if it is usable only by confident, well-resourced or highly specialised users. Human-centred AI evaluation, therefore, asks a different question from conventional technical evaluation. It does not only ask, “Does the model perform?” It asks, “Does the model become safe, usable, trusted and equitable in the system where it is deployed?” The extension of PROLIFERATE to digital evaluation for inter-professional education shows that the same complexity logic can travel across clinical AI, health education, implementation science and policy translation [25].
Implementation is where the argument is tested
The strongest public health test of an argument is whether it changes implementation. This is why the Country Heart Attack Prevention Project matters.
The CHAP implementation study introduced evidence-based, person-centred alternative delivery models for cardiac rehabilitation across rural and remote South Australia, using flexible pathways, including face-to-face, telehealth, telephone, web-based, and primary care options [26]. The evaluation found higher completion, higher patient satisfaction, and lower cost per completed program compared with usual care [26]. Public coverage of the work links these outcomes to South Australia’s new statewide cardiac rehabilitation model of care [7], while the CEIH model describes the policy goal as a coordinated, integrated and accessible cardiac rehabilitation system, especially for rural, remote and Aboriginal communities [27].
The same implementation logic also applies to how evidence is communicated and translated. For example, the same version of this section of the discussion can be offered as a podcast so that readers who prefer to listen can engage with the material in a format that suits them: listen to the CHAP section. This is not only a convenience; it reflects the article’s wider claim that accessibility, format and context shape whether evidence can travel, be understood and become useful, just as flexible delivery models shape participation and outcomes in cardiac rehabilitation.
CHAP matters because it demonstrates that complexity-informed research is neither vague nor anti-practical. It is practical precisely because it refuses to pretend that a single delivery mode, pathway, or outcome measure will fit all people and all contexts. In public health terms, implementation is where equity is tested: who completed, who was satisfied, what it cost, which delivery modes were needed, and how the model could be scaled to statewide care. This is an argument from a successful example. If flexible, person-centred delivery improves completion, satisfaction and cost outcomes in rural and remote cardiac rehabilitation, then public health should not treat flexibility as a compromise. It should treat flexibility as part of the intervention.
The refutation: when linear methods are enough
A fair argument must state when it would be wrong: If a problem is stable, the intervention is clearly defined, the causal pathway is simple, the population is relatively homogeneous, and the context is unlikely to change the result, then linear approaches may be sufficient. In such cases, predefined outcomes, controlled designs and project-based governance may provide efficient and reliable answers.
That is the condition of refutation: The difficulty is that most urgent public health problems do not meet those conditions. They are not stable, context-independent, or experienced equally across populations. Access rules interact with disability and geography. Consumer engagement interacts with power. Continuity of care interacts with culture and trust. Cardiac rehabilitation interacts with biography, networks and service flexibility. AI interacts with workflow, confidence, workload and organisational readiness. When the problem is complex, a method that ignores complexity does not become more rigorous by being simpler. It becomes less fit for purpose.
What must change
The argument can now be stated in full: The claim is that health research must escape linear thinking because linear systems often convert complexity into exclusion. The data come from telehealth access, consumer engagement, transdisciplinary research, First Nations continuity of care, cardiac rehabilitation, fundamental care measurement, clinical AI and rural implementation. The warrant is that complex problems require methods capable of recognising context, relationships, emergence, power and lived experience. The backing comes from PROLIFERATE, PROLIFERATE_AI, the Caring Life Course Theory, and empirical work on consumer engagement, continuity of care and cardiac rehabilitation. The qualifier is that linear methods remain useful for bounded questions. The condition of refutation is that, if a problem is stable, context-independent and causally simple, then linear methods may be enough.
The practical consequences are clear: Funders need to support adaptive evaluation, not only fixed-output projects. Policymakers need to test rules against equity impacts before implementation, not after exclusion becomes visible. Health services need to measure relational and contextual mechanisms, not only throughput and activity. Researchers need to treat consumer and community knowledge as evidence, not as consultation. Digital health and AI programs need to evaluate sociotechnical fit, not only technical performance.
Implementation needs to be understood not as the final step after research, but as the point at which the truth of research is tested. Context is not background; it is part of causality. Relationships are not soft; they are mechanisms. Care is not only a task but also a biography, a network embedded within a person's life course. AI is not only a model or a tech innovation; it is a sociotechnical intervention that affects behaviours and systems. Equity is not a secondary outcome; it is the condition under which public health evidence becomes meaningful.
Conclusion: from control to disciplined learning
Health research stands at a crossroads. One path continues to treat health systems as if they can be improved through discrete projects, predefined outputs and controlled pathways. The other path accepts that health systems are complex, adaptive, relational and political.
The second path is harder. It requires humility, because researchers must accept that they do not fully know the system before entering it. It requires methodological pluralism because no single design can answer every question. It requires a partnership between consumers and the community because lived experience is not merely illustrative; it is explanatory. It requires new forms of accountability, because emergent outcomes may matter more than predefined outputs. It requires courage, because institutions are often more comfortable funding certainty than learning.
The evidence suggests that the second path is more ethical and more effective. Telehealth for homebound people shows how access rules can unintentionally exclude those most in need [2], [3], [20]. Consumer engagement as evidence infrastructure shows that meaningful participation must move beyond consultation [8]. Culturally responsive continuity of care shows that relational and community-adapted care is essential for equity [13]. Care biography and life course care show why care must be understood across biographies, relationships and transitions [15], [16]. Complex adaptive evaluation and human-centred AI evaluation show how evaluation can account for context, uncertainty, usability and system fit [10], [23], [24]. Flexible cardiac rehabilitation implementation shows that person-centred models can improve completion, satisfaction and cost outcomes [26], [7].
The tools, theories and frameworks exist. What is needed now is institutional courage: the courage to fund adaptive research, evaluate emergent outcomes, respect community knowledge, and design systems that learn. The future of public health research should not be organised around the fantasy of control. It should be organised around the discipline of learning with the systems and communities it seeks to change.
Disclosures
This opinion draws on research funded by the Australian National Health and Medical Research Council, Flinders University, and others, as cited here.
Acknowledgements
I thank collaborators across the Caring Futures Institute, Flinders University, the University of Adelaide, the University of South Australia, and national and international partner organisations for their contributions to the research cited here.
Keywords
Transdisciplinary research; knowledge translation; consumer engagement; complexity science; Caring Life Course Theory; telehealth; AI evaluation; health equity; implementation science; First Nations health; homebound people; health marginalisation; PROLIFERATE; PROLIFERATE_AI; cardiac rehabilitation; care biography; fundamental care; social network analysis; wicked problems; post-truth politics.
References
- Tieu M, Lawless M, Hunter SC, Pinero de Plaza MA, Darko F, Mudd A, Yadav L, Kitson A. Wicked problems in a post-truth political economy: a dilemma for knowledge translation. Humanities and Social Sciences Communications. 2023;10:280. doi: 10.1057/s41599-023-01789-6
- Pinero de Plaza MA, Beleigoli A, Mudd A, Tieu M, McMillan P, Lawless M, Feo R, Archibald M, Kitson A. Not well enough to attend appointments: telehealth versus health marginalisation. In: Healthier Lives, Digitally Enabled: Selected Papers from the Digital Health Institute Summit 2020. Amsterdam: IOS Press; 2021. p. 72-79. doi: 10.3233/SHTI210013
- Services Australia. Who can claim telehealth services under MBS or DVA. Updated 11 March 2026. Available from: https://www.servicesaustralia.gov.au/who-can-claim-telehealth-services-under-mbs-or-dva?context=20
- Flinders University ResearchNow. Citation of telehealth systematic review in national policy submission. 2026. Available from: https://researchnow.flinders.edu.au/en/activities/citation-of-telehealth-systematic-review-in-national-policy-submi/
- Australian Government Department of Health, Disability and Ageing. National Strategic Framework for Chronic Conditions 2026-2035. Canberra: Australian Government; 2026. Available from: https://www.health.gov.au/resources/publications/national-strategic-framework-for-chronic-conditions
- Manton T, Dingelstad C, Kovac H, Powell M, Sobels K, Jordan S. Patient experiences of integrated services for chronic disease and social and emotional wellbeing: a case study of the Integrated Team Care Program. Canberra: Australian Institute of Health and Welfare; 2024. Available from: https://www.aihw.gov.au/getmedia/1453fa73-ed0f-40de-ae4c-f06e8a90b017/aihw-imh-24-patient-experiences-of-integrated-services-for-chronic-disease-and-social-and-emotional-wellbeing.pdf?inline=true&v=20250611120752
- Flinders University. New cardiac rehab model could save South Australia up to $10 million a year. Flinders University News. 13 Jun 2026. Available from: https://news.flinders.edu.au/blog/2026/06/13/new-cardiac-rehab-model-could-save-south-australia-up-to-10-million-a-year/
- Wiles LK, Kay D, Luker JA, Worley A, Austin J, Ball A, et al. Consumer engagement in health care policy, research and services: a systematic review and meta-analysis of methods and effects. PLOS ONE. 2022;17(1):e0261808. doi: 10.1371/journal.pone.0261808
- Archibald MM, Lawless MT, de Plaza MAP, Kitson AL. How transdisciplinary research teams learn to do knowledge translation, and how knowledge translation in turn impacts transdisciplinary research: a realist evaluation and longitudinal case study. Health Research Policy and Systems. 2023;21:20. doi: 10.1186/s12961-023-00967-x
- Pinero de Plaza MA, Yadav L, Kitson A. Co-designing, measuring, and optimizing innovations and solutions within complex adaptive health systems. Frontiers in Health Services. 2023;3:1154614. doi: 10.3389/frhs.2023.1154614
- Romera AJ, Bratman EZ, Pinero de Plaza MA, Descalzo AM, Ghneim-Herrera T. Freeing transdisciplinarity from the project straightjacket: reframing the problem. Social Sciences and Humanities Open. 2025;11:101483. doi: 10.1016/j.ssaho.2025.101483
- Archibald M, Ambagtsheer R, Lawless MT, Thompson MO, Shultz T, Chehade MJ, Whiteway L, Sheppard A, Pinero de Plaza MA, Kitson AL. Co-designing evidence-based videos in health care: a case exemplar of developing creative knowledge translation “evidence-experience” resources. International Journal of Qualitative Methods. 2021;20:16094069211019623. doi: 10.1177/16094069211019623
- Pinero de Plaza MA, Gebremichael LG, Brown S, Wu CJ, Clark RA, McBride K, Hines S, Pearson O, Morey K. Health system enablers and barriers to continuity of care for First Nations Peoples living with chronic disease. International Journal of Integrated Care. 2023;23(4):17. doi: 10.5334/ijic.7643
- Beleigoli A, Foote J, Gebremichael LG, Bulamu NB, Astley C, Keech W, Tavella R, Gulyani A, Nesbitt K, Pinero de Plaza MA, et al. Clinical effectiveness and utilisation of cardiac rehabilitation after hospital discharge: data linkage analysis of 84,064 eligible discharged patients, 2016-2021. Heart, Lung and Circulation. 2024;33(7):1036-1045. doi: 10.1016/j.hlc.2024.01.018
- Tieu M, Allande-Cusso R, Collier A, Cochrane T, Pinero de Plaza MA, Lawless M, et al. Care biography: a concept analysis. Nursing Philosophy. 2024;25(3):e12489. doi: 10.1111/nup.12489
- Pinero de Plaza MA, Hutchinson C, Beleigoli A, Tieu M, Lawless M, Conroy T, Feo R, Clark RA, Dafny HA, McMillan P, Allande-Cusso R, Kitson AL. The Caring Life Course Theory: opening new frontiers in care: a cardiac rehabilitation example. Journal of Advanced Nursing. 2025;81(8):5163-5180. doi: 10.1111/jan.16312
- Lawless MT, Wyman C, Pinero de Plaza MA, Block H, George S, et al. Self-care experiences and support needs of community-dwelling older adults with multimorbidity: a qualitative study informed by the Caring Life-Course Theory. Journal of Clinical Nursing. 2026. doi: 10.1111/jocn.70325
- Lawless MT, Pinero de Plaza MA, Thamm C, Kitson A, Paterson C. Applying the Caring Life-Course Theory to explore prostate cancer survivors’ care needs, care trajectories, and self-care behaviors: a qualitative study. Seminars in Oncology Nursing. 2025;41(6):152017. doi: 10.1016/j.soncn.2025.152017
- Lawless MT, Oster C, Block H, Cash B, Bulto LN, Pinero de Plaza MA, George S, Ambagtsheer R, Archibald M, Battersby M, Kitson A. Self-management support interventions for socioeconomically disadvantaged older adults with chronic conditions: a systematic review. Patient Education and Counseling. 2025;141:109305. doi: 10.1016/j.pec.2025.109305
- Pinero de Plaza MA, Gulyani A, Bulto LN, Allande-Cusso R, Pearson V, Lange B, et al. Telehealth as a care solution for homebound people: systematic review and meta-analysis of healthcare utilisation, quality of life, and well-being outcomes. Health and Social Care in the Community. 2025;2025:7224151. doi: 10.1155/hsc/7224151
- Allande-Cusso R, Pinero de Plaza MA, Kitson A, Feo R, Conroy T, Porcel-Galvez AM. How context shapes person-centred fundamental care through nurse-patient relationships: validation of the FoC Intelligence Modelling Tool and predictive pathway analysis. Journal of Advanced Nursing. 2026;82(7):7200-7210. doi: 10.1111/jan.70335
- Allande-Cusso R, Pinero-De Plaza MA, Gomez-Salgado J, Porcel-Galvez AM. Measuring the science of caring: a patient-centred predictive model for the caring interaction. Scandinavian Journal of Caring Sciences. 2025;39(3):e70110. doi: 10.1111/scs.70110
- Pinero de Plaza MA, Lambrakis K, Marmolejo Ramos F, Beleigoli A, Clark R, McMillan P, Morton E, Khan E, Visvanathan R, Chew D, Kitson A, Hendriks J, Barrera-Causil C. PROLIFERATE_AI: a prediction modelling method to evaluate artificial intelligence in meeting end-user-centric goals around better cardiac care. Heart, Lung and Circulation. 2023;32(Suppl 3):S364-S365. doi: 10.1016/j.hlc.2023.06.833
- Pinero de Plaza MA, Lambrakis K, Marmolejo-Ramos F, Beleigoli A. Human-centred AI for emergency cardiac care: evaluating RAPIDx AI with PROLIFERATE_AI. International Journal of Medical Informatics. 2025;196:105810. doi: 10.1016/j.ijmedinf.2025.105810
- Pinero de Plaza MA. Advancing digital evaluation for inter-professional education: a PROLIFERATE_AI mixed-methods analysis. In: Bichel-Findlay J, editor. Health. Innovation. Community: Engage. Disrupt. Transform: Papers from the 29th Australasian Institute of Digital Health’s Health Innovation Community Conference. Amsterdam: IOS Press; 2025. p. 82-86. doi: 10.3233/SHTI251580
- Beleigoli A, Pinero de Plaza MA, Gebremichael LG, Bulamu N, Gulyani A, Chew DP, et al. Implementation of evidence-based, person-centred alternative delivery models for cardiac rehabilitation in a rural and remote population: the Country Heart Attack Prevention Project. Heart, Lung and Circulation. 2026. Online ahead of print. doi: 10.1016/j.hlc.2026.02.008
- Commission on Excellence and Innovation in Health. Statewide Cardiac Rehabilitation Model of Care. Government of South Australia. Available from: https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/clinical+resources/clinical+programs+and+practice+guidelines/medical+conditions/cardiac+care/cardiac+care
- Country Heart Attack Prevention Project. Statewide CR Model of Care. Available from: https://www.chapproject.com.au/outcomes/statewide-cr-model-of-care/
Driven by a focus on innovations that create lasting value, Dr Pinero de Plaza works at the intersection of evaluation, stakeholder alignment, and operational readiness. Through implementation science, she applies dynamic and adaptive strategies, artificial intelligence, and cross-disciplinary methods to move complex ideas beyond pilots and into sustainable adoption.
With a background in Marketing Science, Health Promotion, and Consumer Behaviour, and certified in the Applied AI and Data Science Program (MIT - Massachusetts Institute of Technology), Dr Pinero de Plaza brings a distinctive perspective on how people interact with technologies, environments, and information in complex health and socio-technical contexts. Her work combines behavioural insight, participatory approaches, and systems thinking to evaluate human behaviour, digital innovation, and the responsible integration of AI across disciplines, with proven applications in public health, healthcare interventions, and research and applications on evidence-informed system redesign.
Follow the Topic
-
Health Research Policy and Systems
This journal covers all aspects of the organisation and use of health research – including agenda setting, building health research capacity, and how research as a whole benefits decision makers, practitioners in health and related fields, and society at large.

Related Collections
With Collections, you can get published faster and increase your visibility.
Enabling Environments for Learning Health Systems: Capabilities, Cultures, and Conditions for Learning and Transformation
Health systems globally are under pressure to become learning organizations—capable of generating, sharing, and applying knowledge rapidly and equitably. However, the enabling conditions that make this possible remain under-theorized and inconsistently acted upon.
This Collection invites work that advances the science of enabling environments—the structural, cultural and capability-building conditions that support continuous, adaptive learning within health systems. We welcome conceptual, empirical, and practice-based contributions that explore, examine, and evaluate the enabling environment of learning health systems, including those that deepen collective understanding of the workforce capabilities, organizational cultures, and system conditions that sustain learning in health systems.
Suggested Subtopics
• Culture & Leadership
• Building a culture of curiosity, inclusion and psychological safety
• Roles of leadership and champions in advancing learning
• Embedding equity, patient and caregiver participation in learning practices
• Governance & Policy
• Governance models that promote distributed decision-making and learning
• Policies and incentives that enable experimentation and adaptive improvement
• System-level alignment of priorities, ethics review, and accreditation for learning systems
• Data & Digital Infrastructure
• Data literacy, interoperability and real-time analytics for learning
• Leveraging qualitative and experiential data alongside quantitative measures
• Digital tools and dashboards that support feedback loops and knowledge mobilization
• Funding & Investment Models
• Funding strategies tied to learning goals and long-term capacity building
• Models supporting dedicated time, embedded research roles and sustainability
• Aligning investment with community-identified priorities and system learning cycles
• Knowledge & Capacity Building
• Competency frameworks, continuing education and professional development for learning systems
• Research internships, embedded scientist models and mentorship programmes
• International learning collaboratives, communities of practice and peer-exchange networks
• Practice and Case Studies
• Case studies of health systems operationalizing enabling environments
• Implementation narratives from healthcare organizations, networks, or systems
• Evaluations of learning system maturity or embedded improvement practices
• Methodological Innovations
• Tools and measures for assessing learning system maturity
• Participatory methods, realist evaluation, developmental evaluation in learning systems
• Studies of learning ecosystems and co-design approaches
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Sep 17, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in