A Crisis, A Question, A Program: The Story Behind the PRMD Moral Distress Intervention
Published in Healthcare & Nursing
The Story Behind the Paper
During the COVID-19 pandemic, Iranian hospitals—especially psychiatric wards—became arenas of intense ethical tension. Nurses found themselves trapped between knowing the morally right action and being unable to carry it out because of staff shortages, organizational constraints, overwhelming workloads, or conflicting orders. We witnessed skilled and compassionate nurses experiencing guilt, frustration, powerlessness, and emotional exhaustion as ethical dilemmas multiplied around them.
These real-world challenges raised an urgent question for us:
Why do Iranian nurses experience persistent moral distress, and what kind of intervention—rooted in local culture, conditions, and organizational realities—can truly alleviate it?
Through interviews with front-line nurses, we repeatedly heard stories of unfair workload distribution, poor communication across teams, aggressive patient behavior, hierarchical cultures that silenced nurses, and direct exposure to ethically troubling situations. These encounters were the spark that motivated us to design a structured, culturally grounded program to reduce moral distress.
Conceptual Framing—Bringing Theory to Life
Our study drew upon three guiding perspectives:
-
Professional Nursing Ethics: Highlighting how ethical knowledge, moral sensitivity, decision-making skills, and institutional support can strengthen nurses’ moral resilience.
-
Pragmatic Educational Philosophy: Emphasizing that ethics cannot be taught only through lectures; it must be practiced and reflected upon through real cases, storytelling, and interactive learning.
-
A Multidisciplinary Lens: Integrating medical ethics, nursing management, communication science, and program planning to create a multi-layered intervention.
Our premise was clear:
Moral distress is not caused by a single deficit. It is the result of interconnected individual, managerial, organizational, and relational factors. Only a multi-dimensional intervention can meaningfully reduce it.
Methodology – Systematic Design of an Educational Intervention
To explore this complexity and design a suitable solution, we adopted a multiphase mixed-methods design:
-
Qualitative Phase:
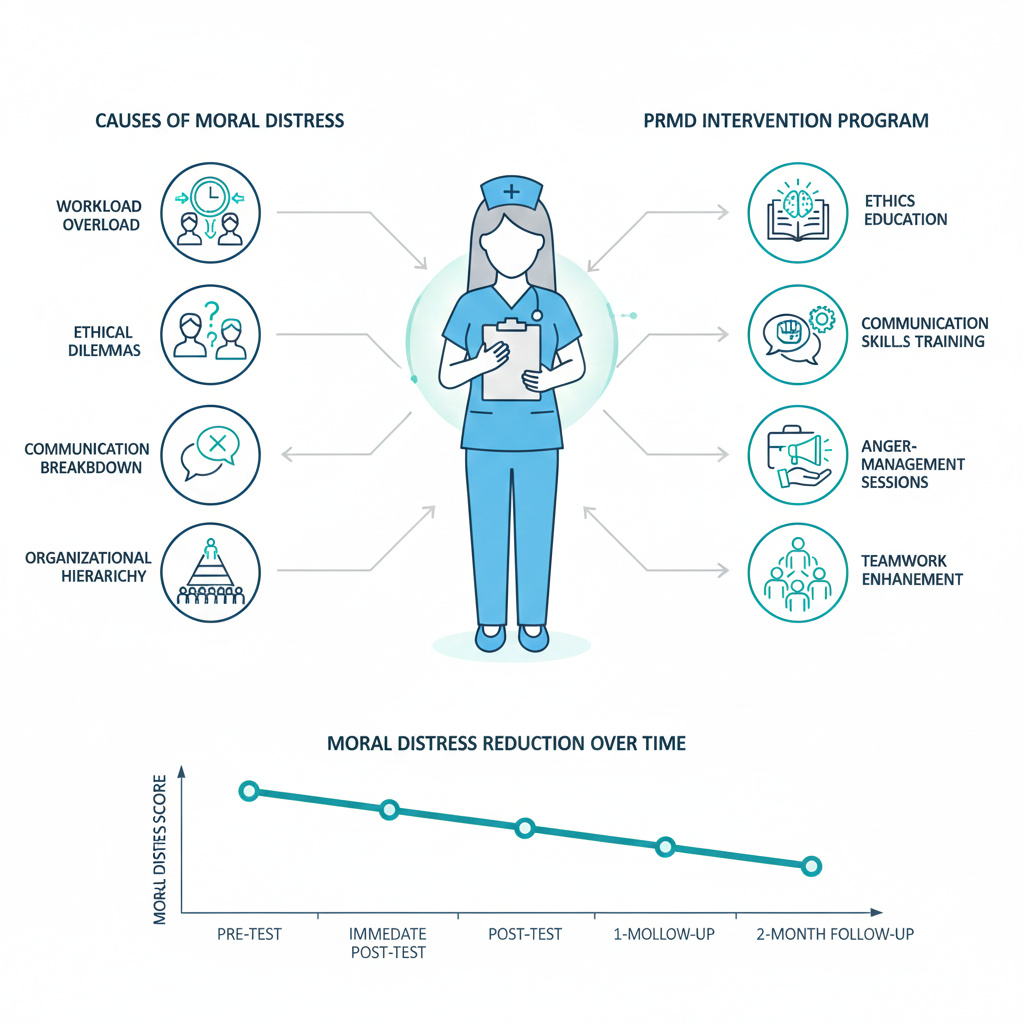
Interviews with 12 nurses revealed the roots of moral distress—deficient professional competency, inadequate communication, hierarchical organizational culture, high workload, poor task allocation, personal ethical uncertainty, and witnessing moral dilemmas. -
Program Design (PRMD):
Using the Ewles & Simnett Model, we developed an intervention that combined educational, managerial, and environmental strategies. Ethics workshops, case-based discussions, communication training, anger-management sessions, moral storytelling, and virtual learning activities were incorporated. -
Program Implementation:
Forty nurses participated in the 3-month program, which included face-to-face classes, virtual sessions, ethics discussions, managerial meetings, and scenario-based exercises. -
Program Evaluation:
Using a pre-test and repeated post-tests alongside a secondary qualitative phase, we assessed the program’s effects at four intervals.
This structured, evidence-driven process allowed us to design a culturally consistent program grounded in both empirical data and practical realities.
Key Findings—What the Evidence Revealed
-
A significant reduction in moral distress:
Quantitative results showed a steady, meaningful decline in the frequency, intensity, and total moral distress scores immediately after the intervention and at one- and two-month follow-ups. -
Moral empowerment of nurses:
Nurses reported improved ethical awareness, stronger decision-making abilities, greater confidence, and a clearer understanding of ethical principles. -
Enhanced ethical climate:
Better workload management, improved task allocation, and greater managerial involvement contributed to a more supportive, fair, and ethical work environment. -
Improved communication and teamwork:
Through discussions, scenario-based learning, and communication training, nurses experienced better interactions with colleagues and patients.
Together, these findings showed that moral distress is not simply an emotional burden—it is shaped by education, culture, management, and workplace structures.
Why This Matters—The Iranian Nursing Lens
Iran’s health system faces chronic nursing shortages, heavy workloads, and hierarchical clinical cultures. Existing international moral distress interventions do not align with local realities: they overlook cultural norms, resource limitations, and ethical expectations specific to Iranian nurses.
Our study is rooted in Iranian nurses’ lived experiences and responds directly to their needs. The PRMD program is one of the first comprehensive, evidence-based, and culturally adapted interventions for reducing moral distress in Iran.
Policy and Practice Implications—Beyond Education
One message is clear:
Moral distress cannot be reduced through education alone. Organizational transformation is essential.
We recommend:
-
Meaningful participation of nurses in clinical and managerial decision-making
-
Establishment of active ethics committees in hospitals
-
Continuous ethics education with real cases and scenarios
-
Redesigning task allocation and workload systems
-
Strengthening interprofessional communication
-
Managerial engagement in creating an ethical climate
These changes can elevate ethical quality, reduce emotional burden, and enhance the well-being of nurses and patients alike.
Why the Timing Matters
Published in 2023, this paper emerged in the aftermath of COVID-19, when nurses had endured unprecedented ethical pressures. The timing is critical: the health system must now rebuild not only its physical capacity but also the moral and psychological resilience of its frontline workforce.
Personal Motivation – A Moral Commitment
For us as researchers, this project was more than an academic endeavor—it was a moral obligation. Iranian nurses navigate complex ethical landscapes with limited support, yet they continue to strive for compassionate and just care. Many shared their pain quietly, without institutional recognition or emotional support.
We felt responsible for amplifying their voices, translating their struggles into evidence, and creating a pathway toward meaningful change.
Conclusion
This study builds bridges between nursing ethics, healthcare management, education, and organizational justice.
We hope it inspires broader conversations and future action towards a workplace where:
no nurse stands alone in ethical distress.
no moral dilemma goes unaddressed.
and ethical practice becomes a shared, supported responsibility.
Follow the Topic
-
BMC Medical Education
This is an open access journal publishing original peer-reviewed research articles in relation to the education and training of healthcare professionals. It welcomes studies on students and professionals across all levels of education; education delivery aspects; and other education-related topics.

Related Collections
With Collections, you can get published faster and increase your visibility.
Lifelong learning and patient safety
BMC Medical Education is calling for submissions to our Collection, Lifelong learning and patient safety. As healthcare delivery becomes increasingly complex, shaped by biomedical advances, digital transformation, demographic shifts, and changing patient expectations, so does the potential for errors and adverse events. This phenomenon makes it essential to equip all healthcare professionals with training and tools to prioritize patient safety across different clinical environments.
Patient safety is a global health priority, with the World Health Organization identifying unsafe care as one of the leading causes of avoidable morbidity and mortality worldwide. While traditional models of competence, validated at a single point in time through licensure or certification, can be valuable, addressing this challenge requires a workforce that is continuously learning, adaptive, and equipped to respond to evolving patient safety threats. Lifelong learning in healthcare plays a pivotal role in fostering patient safety by making sure that healthcare professionals remain competent and adaptive to the best practices in the medical field. Outdated knowledge or skills in the medical field can directly jeopardize patient outcomes. Therefore, continuous professional development allows clinicians to update their professional competencies, reducing the risk of errors and adverse events.
This Collection invites research that examines how patient safety, which should be a professional expectation and ethical imperative at all stages of one’s career trajectory, can be enhanced through innovation in health professions education and training. Topics of interest include, but are not limited to:
• Tools and strategies for integrating patient safety into medical and nursing curricula
• Lifelong learning and continuing professional development (CPD) for patient safety and competence
• Simulation for teamwork, inclusion, and communication in diverse healthcare teams to enhance patient safety
• Interprofessional and collaborative safety culture
• Infection prevention and medication safety practices
• Learning from errors, near-misses, and real-time decision-making in clinical teams
• Strategies and policies for enhancing lifelong learning for patient safety
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 3: Good Health and Well-Being and SDG 4: Quality Education.
Publishing Model: Open Access
Deadline: Aug 18, 2026
Disability in medical education
BMC Medical Education welcomes submissions to our Disability in medical education Collection. As disability impacts so much of our patient population, medical curricula must evolve to address gaps in knowledge, attitudes, and clinical care. Incorporating disability-specific education strengthens inclusive education practices, reduces disparities, and prepares clinicians to deliver person-centered care. Innovative tools, assessments, and instructional approaches, from simulation training to standardized patient encounters to Universal Design for Learning, can be leveraged to improve learners’ understanding of access, communication, ethical, other considerations in clinical practice.
We welcome research covering topics including but not limited to:
• Development and integration of disability curriculum within medical education
• Teaching strategies that promote competency in caring for patients with disabilities
• The role of inclusive education and Universal Design for Learning in clinical training
• Evaluation tools and assessment methods for measuring disability-related knowledge and skills
• Use of patient narratives, simulation, and standardized patients with disabilities in clinical teaching
• Interprofessional education initiatives focused on accessibility and patient-centered care
• Addressing barriers within healthcare training environments
By emphasizing innovation and access, this work supports the development of a medical workforce equipped to deliver compassionate, equitable care for all patients.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 4: Quality Education and SDG 10: Reduced Inequalities.
Publishing Model: Open Access
Deadline: Sep 07, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in