A phage cocktail protects from cholera
Published in Microbiology
Written by Lynne Cairns, Minmin Yen and Andrew Camilli
In 1896, the British scientist Ernest Hankin was studying cholera in the Ganges and Jamuna rivers in India when he observed that certain waters “contained an antiseptic that had a powerful bactericidal action on the cholera germ”. This antiseptic was heat-labile, specific for V. cholerae and retained its activity after filtration. Although he did not know it at the time, Hankin likely identified V. cholerae phages in these waters. It wasn’t until Felix Twort and Frederick d’Herelle independently observed bacterial lysis, in 1915 and 1917, respectively, that bacterial viruses (bacteriophages) were discovered.
The Camilli lab’s own interest in phages began over 10 years ago when Eric Nelson, a graduate student at the time, noticed that clinical rice-water stool (diarrheal) samples from the International Centre for Diarrhoeal Disease Research in Bangladesh contained phages. At first, these phage-containing patient samples were just discarded, since isolating V. cholerae from them was challenging. After persevering further, however, Nelson realized that phages could impact V. cholerae transmission. A few years later, Kimberley Seed, a postdoctoral scholar, identified and characterized three unique lytic phages from cholera patient stool samples (Seed et al. 2011). These phages, named ICP1, ICP2, and ICP3, were found in samples spanning a 10-year period, but all three were never identified in a single sample. These observations prompted our hypotheses that the combinatorial pressures of all three phages might preclude symptomatic infection.
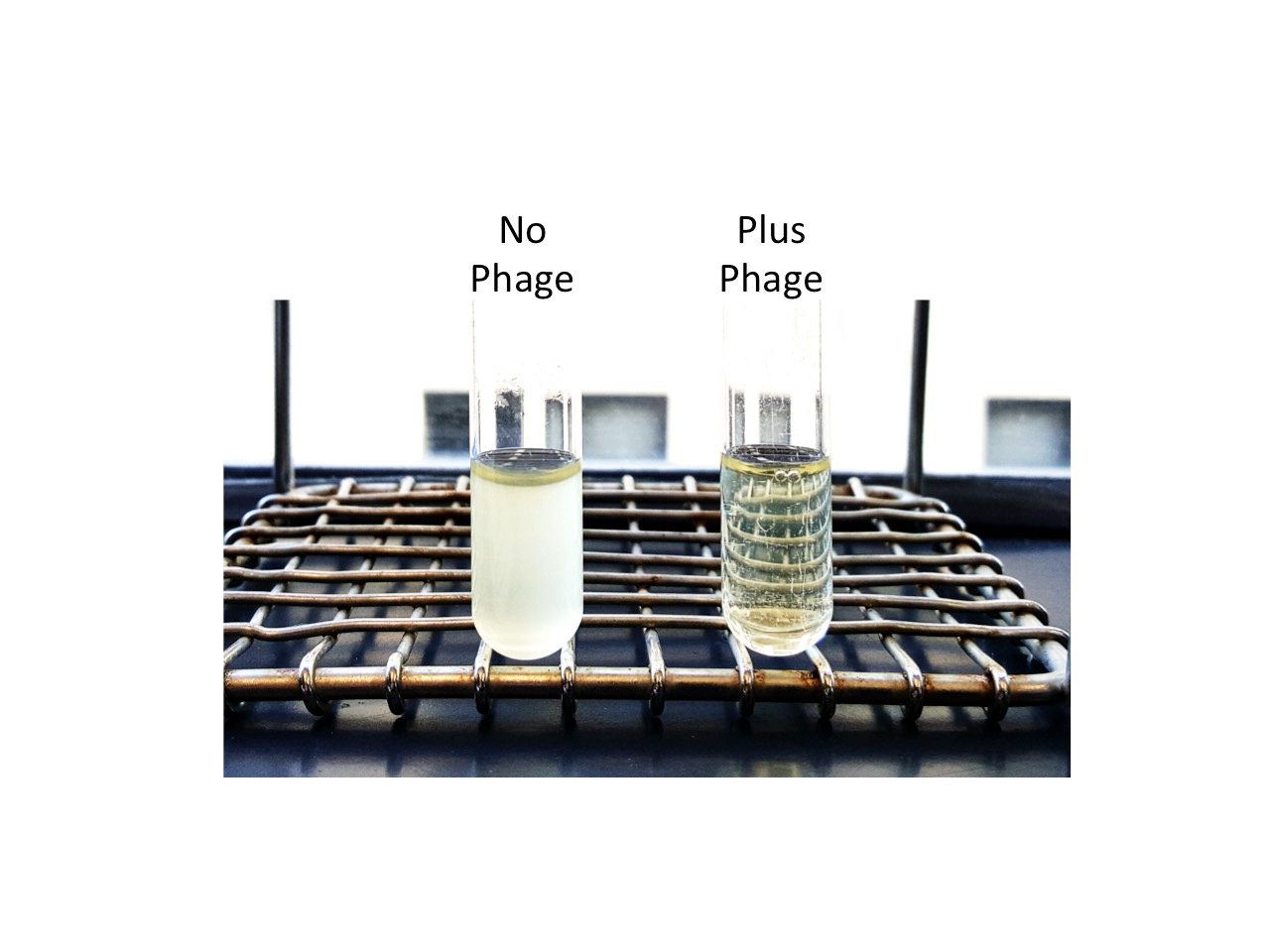
Our work shows that when given up to 24 hours before V. cholerae infection, the ICP cocktail can greatly reduce the V. cholerae burden in the intestinal tract and prevent disease symptoms. When V. cholerae isolates that survived phage prophylaxis were tested for phage resistance, we saw that none of them were resistant to all three phages. When isolates were resistant to a phage, we could usually trace this back to mutations in genes needed for phage receptor production. Satisfactorily, Kimberley Seed's published work showed that such mutations negatively impact V. cholerae virulence. So, although phage predation selects for loss-of-receptor mutants, such mutants are likely avirulent in the host. In other words, V. cholerae is between a rock and a hard place when it is infecting the human intestine in the presence of ICP phages.
So when would phage prophylaxis be most effective? Previous studies have found that cholera can be transmitted very effectively within households (Sugimoto et al. 2014). The peak incidence of cholera in these household contacts occurs a few days after the index patient presents with symptoms. We suggest that phage prophylaxis, integrated alongside the existing prevention and care infrastructure, could present one means of better protecting household contacts.
Unfortunately, phage therapy still faces many challenges before products reach the clinic. While Russia and countries in Eastern Europe have long used phages to treat microbial infections, the Western world’s interest in phage therapy has only risen of late, following the rise of antimicrobial drug resistance. As such, there is currently no regulatory pathway specifically for the application of phages in healthcare settings. Phage therapy presents many advantages, including auto-dosing properties (where the multiplication of phages increases the perceived dose in the patient) and specificity for one bacterial species. We hope our study provides a proof-of-concept that phage therapy can contribute to addressing the global burden of bacterial infections.
See the published paper here: http://rdcu.be/oXHZ
References:



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in