Attitudes and Practice of Health Care Providers Toward Cancer Screening: A Cross‑sectional Multicenter Study, Saudi Arabia
Published in Healthcare & Nursing, Cancer, and Public Health
By 2030, the number of cancer cases worldwide is estimated to increase to 21.4 million deaths due to changes in population demographics. Improved survival can be achieved through cancer prevention and early detection strategies. Accordingly, the new generation may have lower rates of cancer in adulthood than previous generations. Achieving this goal requires a more interdisciplinary and multifaceted approach, with multiple public and clinical health efforts required to build a sustainable infrastructure for the dissemination of cancer prevention interventions.
Recognizing the vital role of health care providers (HCPs) as the most valuable resource for health is fundamental to maintaining public health. At the same time, HCPs must be in good health to treat and care for patients. Although HCPs are constantly exposed to a wide range of health and safety hazards while maintaining the health of the population as a whole, they are not at lower risk of noncommunicable diseases such as cancer.
According to the latest data for 2020, there were an estimated 23,782.8 to 66,899.8 new cases of cancer in Saudi Arabia. The death rate from cancer was estimated at 13,069, with colorectal cancer, lung cancer, and breast cancer being the leading causes. Although there is significant research on overall cancer incidence and prevalence in Saudi Arabia, there is a lack of data on the perceptions and attitudes of health care providers regarding their decision to undergo cancer screening. Therefore, we aimed to assess the perceptions and personal attitudes of n = 372 HCPs regarding their decision to undergo cancer screening.
We found that regardless of gender, occupation or age, the overall level of belief in the protective value of regular cancer screening was high at 91.4%. However, only 3.5% of participants had undergone colonoscopy and only 15.9% of women had undergone mammography, while the percentage of men who had undergone prostate-specific antigen (PSA) screening was 12.4%. At the same time, we found that the number of women in the 45-54 age group who were screened with mammography was significantly higher than those who were not screened. Similarly, the number of male physicians over 54 years who were screened for PSA was significantly higher than those who were not.
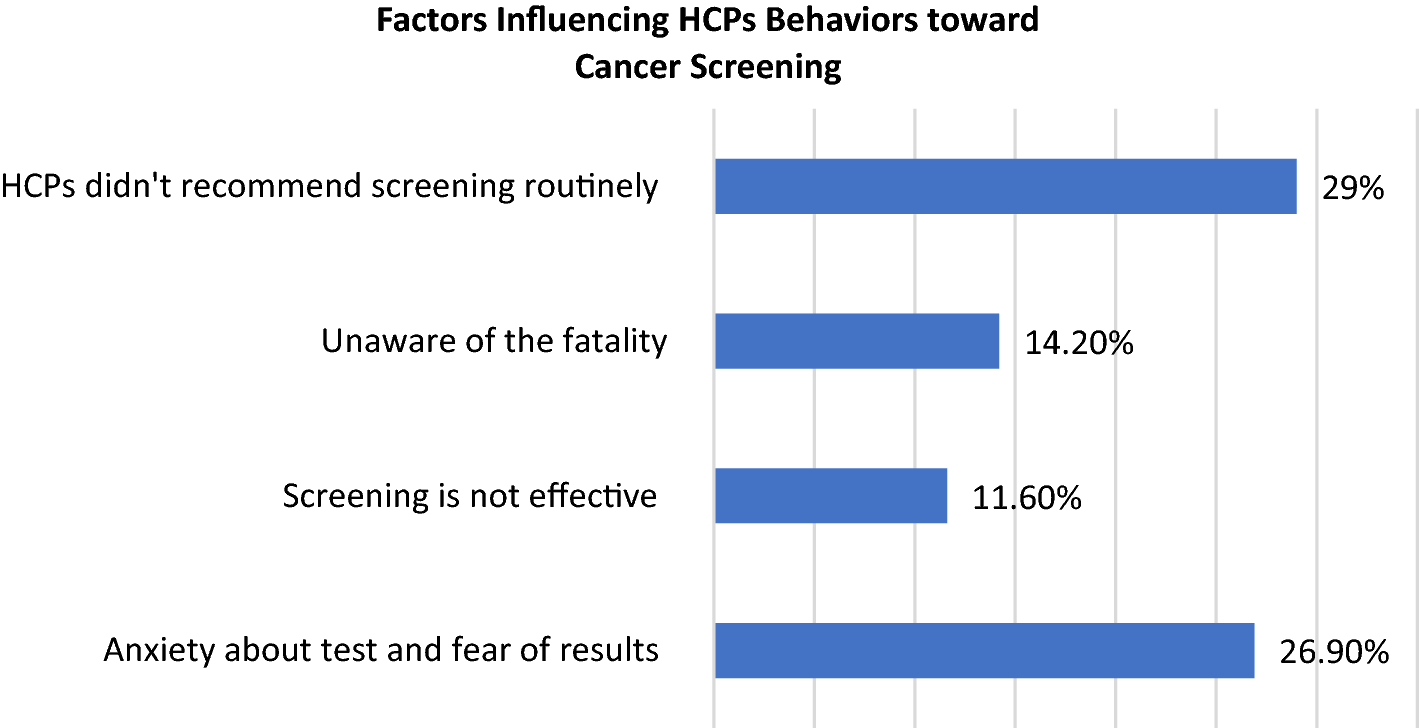
The most common reason respondents cited that influenced their decision to undergo cancer screening was the lack of knowledge. The second most common reason that participants cited that influenced their decision to undergo screening was worry and anxiety about receiving positive results. Therefore, educational programs are recommended, especially among physicians, as they can further inform their patients about cancer risk factors, the importance of cancer screening, and the differences between screening methods.
The results of the current study and the available evidence specifically regarding the Saudi community indicate a need for awareness raising, emphasizing the role of HCPs in motivating themselves, their families and their patients to implement various cancer screening programs. This could be achieved through further research into additional education or training required for HCPs, which could positively influence their attitude towards cancer screening by making the procedure part of their own routine medical check-up.
Follow the Topic
-
Journal of Epidemiology and Global Health
The journal aims to impact global epidemiology and international health with articles focused on innovative scholarship and strategies to advance global health policy.

Related Collections
With Collections, you can get published faster and increase your visibility.
Climate and Environmental Change as Drivers of Infectious Disease: A Planetary Health Perspective
Human health is increasingly shaped by the interconnected pressures of climate change, environmental degradation, and socio‑ecological disruption. These planetary‑scale changes influence not only the epidemiology of infectious diseases, but also the public health systems, social structures, and community capacities that determine exposure, vulnerability, and resilience. This Collection adopts a planetary health perspective to explore how climate variability, ecosystem disruption, and human–environment interactions affect infectious disease risks and the public health responses needed to address them.
We welcome research that examines how shifts in temperature, precipitation, humidity, extreme weather events, land‑use change, biodiversity loss, and urbanization influence pathogen ecology, transmission pathways, and population vulnerability. Beyond epidemiological patterns, the Collection seeks contributions that address preparedness, surveillance, health system resilience, risk communication, governance, and cross‑sectoral interventions aimed at mitigating and adapting to climate‑related infectious disease threats.
Studies leveraging epidemiological datasets, climate and environmental records, spatial mapping, and predictive modeling are encouraged, as are qualitative, policy‑focused, and implementation‑oriented works that illuminate barriers and opportunities within public health systems. Particular attention is given to inequities in exposure and resilience, the needs of high‑risk populations, and the role of community‑level and institutional adaptation strategies.
By integrating epidemiology, environmental science, and public health practice, this Collection aims to advance understanding of climate–disease interactions, strengthen early warning and response systems, and inform adaptive strategies that protect and promote planetary health in a rapidly changing world. Topics of interest include but are not limited to:
- Climate‑sensitive infectious diseases and changing transmission patterns
- Impacts of extreme weather events and environmental disruption on disease risk
- Public health preparedness, surveillance, and early warning systems
- Health system resilience and climate adaptation strategies
- Socio‑ecological vulnerability, inequities, and community resilience
- Land‑use change, biodiversity loss, and zoonotic spillover
- Modeling climate, environmental, and disease interactions
- Governance, policy, and multisectoral responses to planetary health threats
- One Health and Planetary Health approaches to infectious disease prevention
This Collection supports and amplifies research related to SDG 13, Climate actions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 31, 2027
Public Health Professionals’ Education
Strengthening the education and continuous professional development of public health professionals is fundamental to achieving resilient, equitable, and responsive health systems. Recent global experiences including pandemics, protracted humanitarian crises, climate-related health risks, rapid urbanization, and technological transformation have highlighted both the critical role of the public health workforce and persistent gaps in training relevance, scale, quality, and sustainability. In many settings, educational models remain insufficiently aligned with real-world system needs, emerging competencies, and evolving career pathways.
While there is growing innovation in public health education, evidence and lessons learned are dispersed across disciplines and regions. A focused supplement in the Journal of Epidemiology and Global Health will provide a timely scholarly platform to consolidate high-quality research and practice-based insights.
The proposed Collection aims to advance knowledge in the education of public health professionals by:
Showcasing empirical evidence and innovative models for public health education and training
Examining how educational approaches align with health system priorities and workforce needs
Informing policy, institutional strategies, and investment in public health workforce development
Promoting equity, quality, and sustainability in public health education globally.
Scope and Thematic Areas
The supplement will invite original research articles, systematic or scoping reviews, and rigorously documented practice-based papers across the following thematic areas:
Competency-Based Public Health Education
- Core and advanced competency frameworks
- Alignment of curricula with population health needs and system priorities
Field-Based and Applied Learning Models
- Field Epidemiology Training Programs (FETPs) and similar applied training models
- Experiential learning, service-based education, and community engagement
Interprofessional and Multisectoral Education
- Collaborative training across health, social, environmental, and humanitarian sectors
- Preparing public health professionals for whole-of-government and whole-of-society approaches
Digital, Blended, and Distance Learning Innovations
- Online and hybrid training models
- Use of digital platforms, simulation, and emerging technologies in education
Education for Health Emergencies and Fragile Settings
- Workforce training for outbreak preparedness, humanitarian response, and conflict settings
- Adaptive education models in fragile and resource-constrained contexts
Equity, Ethics, and Inclusion in Public Health Training
- Gender, geographic, and socioeconomic equity in access to education
- Ethical dimensions of training, mentorship, and professional advancement
Leadership, Management, and Systems Thinking
- Training for public health leadership, governance, and policy engagement
- Building managerial and strategic competencies for system-level impact
Mentorship, Supervision, and Career Pathways
- Structured mentorship and supervision models
- Transition from training to practice and career progression
Monitoring, Evaluation, and Impact of Public Health Education
- Methods for assessing educational outcomes and workforce impact
- Long-term sustainability and return on investment of training programs
Partnerships, Financing, and Institutionalization
- Academic–government–partner collaborations
- Financing models and institutional integration of training programs
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Dec 17, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in