Behind the Paper: Implementing a closed loop clinical decision support system for sustainable preoperative care
Published in Computational Sciences, Pharmacy & Pharmacology, and Business & Management
Publishing in a Q1 journal is a goal that seems almost unattainable when you are a resident or even a staff physician. It’s easy to believe that such an achievement requires a groundbreaking contribution to the scientific community, for example inventing a revolutionary device for difficult intubations, a new broad-spectrum antibiotic, or an intravenous drip which automatically calculates the dose of intravenous fluids in real time. Yet, according to the famous words of John Lennon, “Life is what happens to you while you’re busy making other plans.” Unexpectedly, I find myself writing about a project that, while less dramatic, has had a profound impact on quality of care and healthcare expenditure in our anesthesiology department.
This initiative is part of a broader effort to develop a remote digital preoperative evaluation system that is not only more efficient than conventional methods but also allows anaesthetists to dedicate more time to the operating room. Healthcare systems face critical challenges worldwide, including lack of resources and increased demand, making significant structural reforms an urgent need. However, rigid legal frameworks often hinder the evolution of medical processes, due to a unfounded belief that financial resources alone can sustain healthcare systems. Evidence shows that such static approaches are destined to fail. As members of the healthcare sector, it is our duty to identify and resolve process inefficiencies.
Every innovation begins somewhere, and emergency situations, such as the COVID-19 pandemic, can accelerate the need for change. In Spain, in the months prior to the pandemic’s onset, our team had already started collaborating with IT staff to refine the criteria for pre-surgical complementary tests. The aim was to encourage appropriate preoperative testing through a streamlined checklist, developed by standardizing surgical interventions and matching complementary tests with patient physical status and surgical risk (ASA scale).
During the lockdown in March and April 2020, the ICU volume tripled, and all anaesthetists at our center were assigned to critical care. Meanwhile, patients with urgent oncological, neurological, or other serious conditions faced surgical delays, with many being hesitant to visit hospitals or unable to access care due to restrictions. At the same time, physicians were encouraged to avoid face-to-face care. Faced with this challenge, we recognized the necessity of a system that could meet the needs of both patients and physicians.
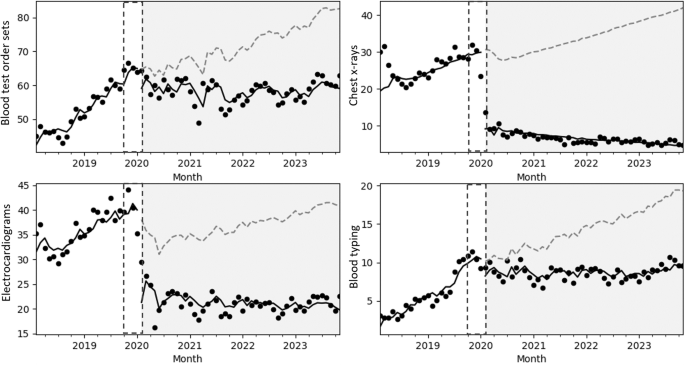
The solution was the development of a remote digital pre-anaesthesia consultation system, including the published intervention which seeks to reduce unnecessary preoperative testing, with obvious benefits for patient safety, quality of life, and healthcare expenditure. At the same time, we also deployed a value-based, virtually supervised pre-operative evaluation program. Looking ahead, we aim to publish details of this innovative circuit in early 2025. Meanwhile, we reflect on a critical lesson: stagnation in obsolete and inefficient systems is not an option. We must embrace new technologies, including artificial intelligence and digital platforms, to create a continuously evolving healthcare system. Our ultimate goal is to integrate innovation seamlessly into daily practice to benefit patients, healthcare professionals, and health systems alike.
Anesthesiologist, MD, Ph D. 20 years in Surgerý room, 8 as Chieff of staff and Director of Surgeries. Currently sharing my work in theaters with Hospital management as Hospital Medical Director.
I'm currently very interested in developing methods to do things right, with minimum effort and maximum revenue. People over all things.
Follow the Topic
-
npj Digital Medicine
An online open-access journal dedicated to publishing research in all aspects of digital medicine, including the clinical application and implementation of digital and mobile technologies, virtual healthcare, and novel applications of artificial intelligence and informatics.

Related Collections
With Collections, you can get published faster and increase your visibility.
Synthetic Clinical Data and Privacy-Preserving Frameworks for Trustworthy Health AI
Publishing Model: Open Access
Deadline: Jun 03, 2027
Digital Biomarkers for Enabling Proactive Clinical Decisions
Publishing Model: Open Access
Deadline: May 18, 2027



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in