Classification of distinct tendinopathy subtypes for precision therapeutics
Published in Biomedical Research
Rotator cuff tendinopathy is an extremely common musculoskeletal disorder, characterized by shoulder pain and discomfort in daily activities such as dressing, combing hair, or lifting heavy objects. Traditional treatment methods are often empirical, focusing primarily on symptom relief, including corticosteroid injections, rehabilitation therapy, and even surgery. However, many patients do not achieve lasting relief and instead find themselves caught in a cycle of repeated treatments. Why does the same treatment work for some but not for others?
For a long time, corticosteroid therapy has been the cornerstone of tendinopathy treatment1, with its pain-relieving effects being almost immediate following injection. However, there remains ongoing debate regarding its long-term efficacy. Corticosteroid injections for rotator cuff tendinopathy can reduce pain and improve functionality in the short term2, yet these benefits do not necessarily translate into a reduced risk of requiring surgical intervention in the future1. Additionally, whether corticosteroids affect tendon healing after rotator cuff repair remains controversial. Some studies suggest that preoperative steroid use may be associated with an increased risk of postoperative rotator cuff retears3, while other studies argue that corticosteroids do not elevate the risk of retear4. Clinicians in our team have also encountered similar dilemmas in practice. We are uncertain about when corticosteroids should be used, which patients might benefit from corticosteroid therapy, and which patients might not require it.
To address this issue, our research team proposed that rotator cuff tendinopathy may not be a single disease, but rather a condition with distinct subtypes. Identifying these subtypes and developing targeted treatments for each subtype may enhance clinical outcomes. In our previous work on osteoarthritis (OA), we used a big data approach and employed unsupervised clustering analysis to identify four subtypes of OA based on the transcriptomic profiles of cartilage samples. These subtypes showed strong correlations with clinical symptoms and imaging evidence. More importantly, when we categorized all known therapeutic drugs for OA, we found that these treatments aligned well with the four identified OA subtypes. This subtype classification thus holds significant potential to guide more precise clinical diagnosis and treatment for OA.
We were inspired by this study and subsequently reviewed a substantial amount of related literature. We discovered that in research on various heterogeneous diseases, transcriptomic sequencing techniques have proven valuable for personalized treatment by revealing the molecular heterogeneity of diseases. By identifying distinct molecular subtypes in different patients, it is possible to tailor more precise treatment strategies, thereby enhancing therapeutic effectiveness and reducing unnecessary side effects.
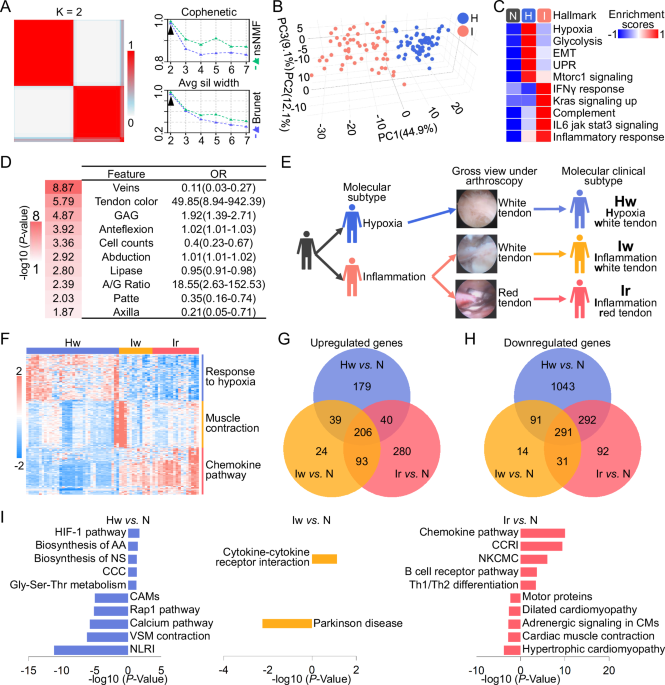
In our study, we collected clinical samples from 126 diseased tendons and performed transcriptomic sequencing. Through unsupervised clustering, we identified two distinct molecular subtypes, which we named the H and I subtypes based on their unique molecular characteristics. Additionally, we compared the clinical data of patients with these two subtypes. As we were preparing to report our findings according to these two subtypes, Professor Ouyang pointed out an intriguing feature within the clinical data: the red, inflamed appearance of tendons observed through arthroscopy. Specifically, 94.7% of red hyperemia tendons were identified as Subtype I, while 73.5% of white non-hyperemia tendons were Subtype H. Professor Ouyang suggested that we should further refine the molecular subtyping by incorporating the arthroscopic appearance of tendon. This approach, combining both molecular and clinical features, would make the classification more practical and accessible for future clinical applications.
Based on transcriptomics and clinical pathological characteristics, we identified and characterized three distinct subtypes of rotator cuff tendinopathy. The hypoxic atrophic subtype with a white appearance (Hw) significantly downregulated angiogenesis pathways and upregulated hypoxia, glycolysis, and cartilage-related pathways. In contrast, other subtypes mainly exhibited upregulation of inflammatory and proliferative pathways. The inflammatory proliferative subtype with a white appearance (Iw) only showed moderate upregulation of inflammatory and proliferative characteristics. The inflammatory proliferative subtype with a red appearance (Ir) exhibited the highest levels of angiogenesis and inflammatory pathway upregulation, accompanied by the most severe joint dysfunction. Our research team further established research models targeting tendon disease subtypes, including specific subtype animal model simulations and clinical data analysis, which validated the widely used but controversial therapy—corticosteroid treatment—can only reverse the pathological characteristics of the high-inflammatory proliferative subtype, thereby improving prognosis. The findings of this study are expected to advance the progress of basic research related to rotator cuff tendinopathy subtypes and the implementation of precise clinical treatment.
.png)
[1] Mohamadi A, Chan J J, Claessen F M, et al. Corticosteroid Injections Give Small and Transient Pain Relief in Rotator Cuff Tendinosis: A Meta-analysis [J]. Clin Orthop Relat Res, 2017, 475 (1):232.
[2] Lin M T, Chiang C F, Wu C H, et al. Comparative Effectiveness of Injection Therapies in Rotator Cuff Tendinopathy: A Systematic Review, Pairwise and Network Meta-analysis of Randomized Controlled Trials [J]. Arch Phys Med Rehabil, 2019, 100 (2):336.
[3] Puzzitiello R N, Patel B H, Forlenza E M, et al. Adverse Impact of Corticosteroids on Rotator Cuff Tendon Health and Repair: A Systematic Review of Basic Science Studies [J]. Arthrosc Sports Med Rehabil, 2020, 2 (2):e161.
[4] Kim Y S, Jin H K, Lee H J, et al. Is It Safe to Inject Corticosteroids Into the Glenohumeral Joint After Arthroscopic Rotator Cuff Repair? [J]. Am J Sports Med, 2019, 47 (7):1694.
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Tumor Microenvironment Crosstalk and Therapeutic Implications
Publishing Model: Hybrid
Deadline: Nov 02, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in