Epidemiology of Vascular Thrombosis in the Eastern Province of Saudi Arabia: Comparison with National Data
Published in General & Internal Medicine

There is currently no thrombosis registry in the Kingdom of Saudi Arabia, and although the exact prevalence of deep vein thrombosis (DVT) is unknown, it is estimated that 25,000 people suffer from thrombosis. It is well established that thrombophilia is a predisposition to develop venous thromboembolism (VTE) due to an underlying hypercoagulable state caused by inherited or acquired disorders of coagulation or fibrinolysis. Inherited disorders include deficiencies of natural anticoagulants such as antithrombin, protein C, protein S, elevated levels of coagulation factors (especially factor VIII), and prothrombotic polymorphisms in the genes encoding factor V (i.e., factor V Leiden) and prothrombin. Acquired conditions mainly include antiphospholipid antibody syndrome, malignancies, acquired increases in coagulation factors or acquired decreases in natural inhibitors, and hyperhomocysteinemia.
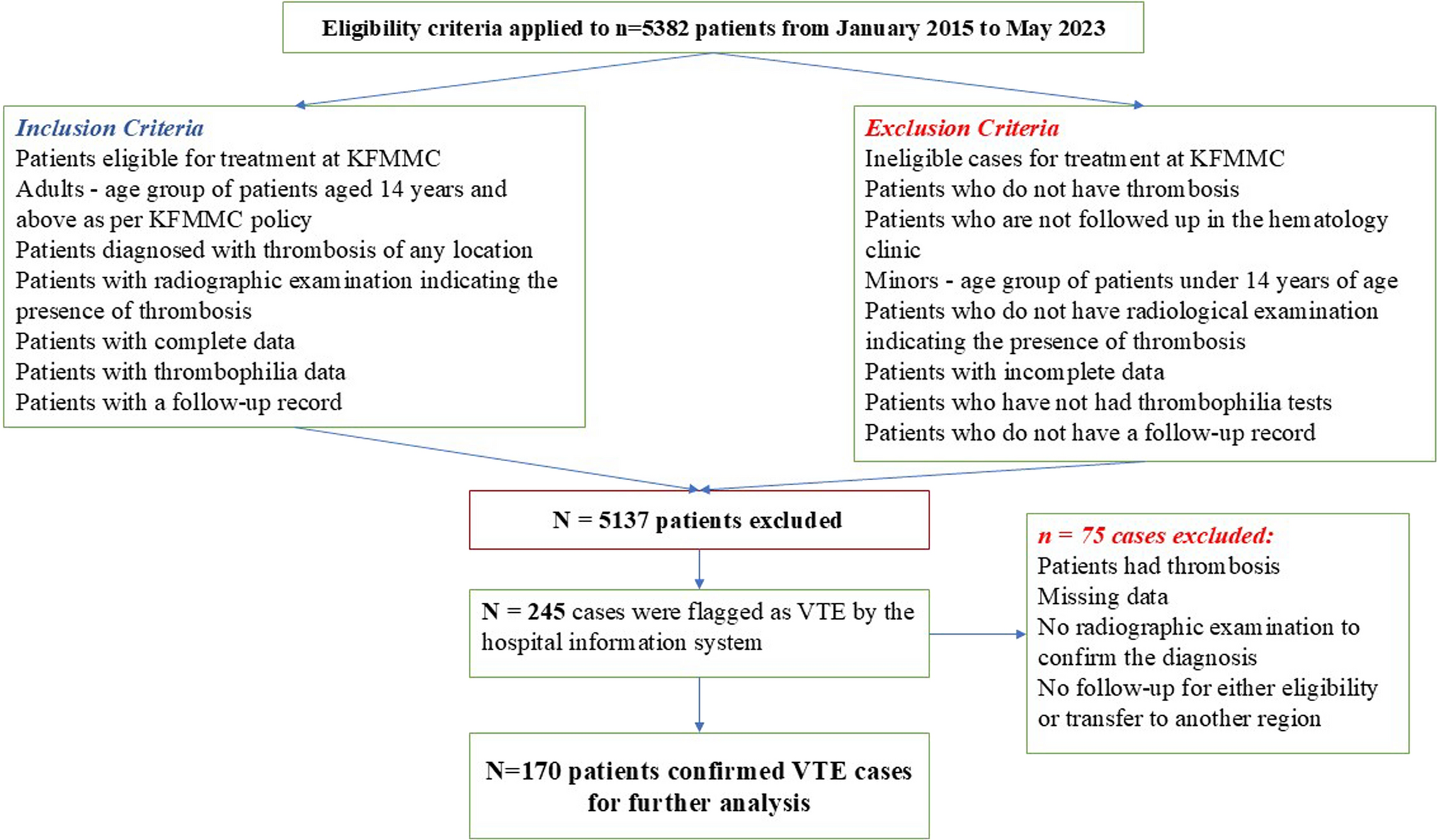
Despite the growing evidence of thrombophilia in the Saudi population across its regions, there have been no studies on thrombotic events in the Eastern Province of Saudi Arabia, the largest province by area and the most obese region (29.4%), followed by Riyadh (26.9%), while the lowest was Baha (14.3%). This study became the first that aimed to investigate the prevalence of VTE in a hematology clinic in the Eastern Province of Saudi Arabia and compare them with national data. The study was conducted at a tertiary care hospital of King Fahd Military Medical Complex (KFMMC) among n = 170 patients seen in the outpatient clinic between January 2015 and May 2023 who were diagnosed with arterial or venous thrombosis, or both.
It was found that with a mean population age of 42.21 (± 13.022), the prevalence of VTE was 3.16%. Since females constituted 70% of the sample, most cases of VTE were in females, which is consistent with some regional studies within Saudi Arabia. Thus, as shown by the studies from Madinah and the Central Province of Saudi Arabia, the female to male ratio was 2:1. On the other hand, in the Southern Province and Jeddah (Western Province) of Saudi Arabia, the ratio was 1:1. Moreover, the results of the current study are inconsistent with global evidence. Accordingly, it would be erroneous to conclude that females are more likely to develop VTE than males, but it is reasonable to further study this relationship in the future to allow emerging patterns.
The smoking rate (12.9%) in this cohort was high compared to other comparable national data. Given the differences in genetic and ethnic distribution, compared to conflicting data from domestic and international sources, this suggests that active smoking is a possible risk factor for VTE in the Eastern Province of Saudi Arabia.
Obesity-related chronic inflammation and decreased fibrinolysis appear to be two major mechanisms of thrombus formation in obesity. In this study, of n=170 patients, 80.5% were overweight or obese, which confirms national data indicating a high prevalence of obesity and overweight as risk factors for VTE. Moreover, this study showed a significantly higher rate compared to other regional studies in Saudi Arabia.
Further findings showed that the most common causes were rheumatological and autoimmune diseases (39.4%), pregnancy (13.5%), prolonged immobilization (12.4%), positive family history of thrombosis (13%), and oral contraceptives or hormonal therapy (8.8%). These figures were significantly higher compared to regional studies in Saudi Arabia. On the other hand, cancer was more common in Medina, Jeddah, and the Southern Province compared to the Eastern Province, while in the Central Province there was no evidence that cancer was a cause of thrombosis. However, longer hospital stay and VTE as postoperative complications were significantly more common in the Central and Southern Provinces compared to the Eastern Province. Further comparative studies in this area are needed to examine the difference in the incidence of postoperative VTE between the Eastern Province and the Central and Southern Provinces. This may indicate that the postoperative approach and the incidence of in-hospital VTE are lower than other regions, with stricter adherence to preventive measures to prevent postoperative VTE.
The most common comorbidities were cardiac disease, chronic kidney disease (CKD), hypertension (HTN), and type 2 diabetes mellitus, which is consistent with earlier studies in Saudi Arabia. However, compared with the data from Madinah, the data from this study showed a significantly higher rate of comorbidities. Regarding recurrent thrombosis, the results of this study conducted in the Eastern Province showed significantly higher rates compared with other regions of Saudi Arabia. It is important to emphasize that earlier studies in Saudi Arabia did not provide any information on dyslipidemia and VTE to compare with the data from the current study. However, based on existing evidence and current research, lifestyle changes and control of blood glucose, blood pressure, cholesterol, triglycerides, and weight loss may reduce the risk of VTE.
Since there are no recent national or global rates for VTE, determining accurate national data is a matter of further multicenter studies across the Kingdom of Saudi Arabia to substantiate the findings of the current study. In addition, additional improvement efforts and a strategic treatment approach are needed to reduce the factors contributing to VTE in the Eastern Province. Developing an awareness program and supporting lifestyle changes are a critical first step to informing people about VTE and how to reduce its risk.
Follow the Topic
-
Journal of Epidemiology and Global Health
The journal aims to impact global epidemiology and international health with articles focused on innovative scholarship and strategies to advance global health policy.

Related Collections
With Collections, you can get published faster and increase your visibility.
Climate and Environmental Change as Drivers of Infectious Disease: A Planetary Health Perspective
Human health is increasingly shaped by the interconnected pressures of climate change, environmental degradation, and socio‑ecological disruption. These planetary‑scale changes influence not only the epidemiology of infectious diseases, but also the public health systems, social structures, and community capacities that determine exposure, vulnerability, and resilience. This Collection adopts a planetary health perspective to explore how climate variability, ecosystem disruption, and human–environment interactions affect infectious disease risks and the public health responses needed to address them.
We welcome research that examines how shifts in temperature, precipitation, humidity, extreme weather events, land‑use change, biodiversity loss, and urbanization influence pathogen ecology, transmission pathways, and population vulnerability. Beyond epidemiological patterns, the Collection seeks contributions that address preparedness, surveillance, health system resilience, risk communication, governance, and cross‑sectoral interventions aimed at mitigating and adapting to climate‑related infectious disease threats.
Studies leveraging epidemiological datasets, climate and environmental records, spatial mapping, and predictive modeling are encouraged, as are qualitative, policy‑focused, and implementation‑oriented works that illuminate barriers and opportunities within public health systems. Particular attention is given to inequities in exposure and resilience, the needs of high‑risk populations, and the role of community‑level and institutional adaptation strategies.
By integrating epidemiology, environmental science, and public health practice, this Collection aims to advance understanding of climate–disease interactions, strengthen early warning and response systems, and inform adaptive strategies that protect and promote planetary health in a rapidly changing world. Topics of interest include but are not limited to:
- Climate‑sensitive infectious diseases and changing transmission patterns
- Impacts of extreme weather events and environmental disruption on disease risk
- Public health preparedness, surveillance, and early warning systems
- Health system resilience and climate adaptation strategies
- Socio‑ecological vulnerability, inequities, and community resilience
- Land‑use change, biodiversity loss, and zoonotic spillover
- Modeling climate, environmental, and disease interactions
- Governance, policy, and multisectoral responses to planetary health threats
- One Health and Planetary Health approaches to infectious disease prevention
This Collection supports and amplifies research related to SDG 13, Climate actions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 31, 2027
Public Health Professionals’ Education
Strengthening the education and continuous professional development of public health professionals is fundamental to achieving resilient, equitable, and responsive health systems. Recent global experiences including pandemics, protracted humanitarian crises, climate-related health risks, rapid urbanization, and technological transformation have highlighted both the critical role of the public health workforce and persistent gaps in training relevance, scale, quality, and sustainability. In many settings, educational models remain insufficiently aligned with real-world system needs, emerging competencies, and evolving career pathways.
While there is growing innovation in public health education, evidence and lessons learned are dispersed across disciplines and regions. A focused supplement in the Journal of Epidemiology and Global Health will provide a timely scholarly platform to consolidate high-quality research and practice-based insights.
The proposed Collection aims to advance knowledge in the education of public health professionals by:
Showcasing empirical evidence and innovative models for public health education and training
Examining how educational approaches align with health system priorities and workforce needs
Informing policy, institutional strategies, and investment in public health workforce development
Promoting equity, quality, and sustainability in public health education globally.
Scope and Thematic Areas
The supplement will invite original research articles, systematic or scoping reviews, and rigorously documented practice-based papers across the following thematic areas:
Competency-Based Public Health Education
- Core and advanced competency frameworks
- Alignment of curricula with population health needs and system priorities
Field-Based and Applied Learning Models
- Field Epidemiology Training Programs (FETPs) and similar applied training models
- Experiential learning, service-based education, and community engagement
Interprofessional and Multisectoral Education
- Collaborative training across health, social, environmental, and humanitarian sectors
- Preparing public health professionals for whole-of-government and whole-of-society approaches
Digital, Blended, and Distance Learning Innovations
- Online and hybrid training models
- Use of digital platforms, simulation, and emerging technologies in education
Education for Health Emergencies and Fragile Settings
- Workforce training for outbreak preparedness, humanitarian response, and conflict settings
- Adaptive education models in fragile and resource-constrained contexts
Equity, Ethics, and Inclusion in Public Health Training
- Gender, geographic, and socioeconomic equity in access to education
- Ethical dimensions of training, mentorship, and professional advancement
Leadership, Management, and Systems Thinking
- Training for public health leadership, governance, and policy engagement
- Building managerial and strategic competencies for system-level impact
Mentorship, Supervision, and Career Pathways
- Structured mentorship and supervision models
- Transition from training to practice and career progression
Monitoring, Evaluation, and Impact of Public Health Education
- Methods for assessing educational outcomes and workforce impact
- Long-term sustainability and return on investment of training programs
Partnerships, Financing, and Institutionalization
- Academic–government–partner collaborations
- Financing models and institutional integration of training programs
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Dec 17, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in